Our top priority is providing value to members. Your Member Services team is here to ensure you maximize your ACS member benefits, participate in College activities, and engage with your ACS colleagues. It's all here.
Membership Benefits
Find a Surgeon
Find a Hospital or Facility
Quality Programs
Education Programs
Member Benefits
Publications
ACS Case Reviews in Surgery
ACS Case Reviews
ACS Case Reviews in Surgery is a unique, peer-reviewed, open access, online-only case report journal published six times a year that presents high-quality, in-depth analyses of actual surgical cases. The journal boasts an exceptional editorial and reviewer board comprised of distinguished surgeon leaders from around the world.
Here are just a few features of this innovative journal:
Each issue features 20 case reports from an extensive array of surgical specialties, including breast, colorectal, pediatric, trauma, bariatric, general, and rural surgery
Full article PDFs of each case report
Option to purchase an annual CME subscription for up to 24 AMA PRA Category 1 Credits ™ (4 credits per issue)
Are you an author? Submit your manuscript online.
Submit a Case Review
Author instructions.
Interested in submitting to ACS Case Reviews in Surgery? Review the requirements your report must meet for submission.
Reviewer Instructions
To be eligible for peer review, all submissions must meet at least one of the list of requirements detailed
Sample Article Submission
Before you submit your case to ACS Case Reviews in Surgery, look over this sample article to familiarize yourself with the format.
Get to Know ACS Case Reviews in Surgery
Gerald A. Isenberg, MD, FACS, Editor-in-Chief, ACS Case Reviews in Surgery, discusses the open access online journal's range of topics and how to submit case reports for publication.
Search ACS Case Reviews in Surgery
Do you have any questions.
Contact and staff information for ACS Case Reviews in Surgery is available.
This website is intended for healthcare professionals
Abbott TEF, Fowler AJ, Dobbs TD Frequency of surgical treatment and related hospital procedures in the UK: a national ecological study using hospital episode statistics. British Journal of Anaesthesia.. 2017; 119:(2)249-257 https://doi.org/10.1093/bja/aex137
American Society of Anesthesiologists. ASA physical status classification system. 2019. https://www.asahq.org/standards-and-guidelines/asa-physical-status-classification-system (accessed 26 August 2020)
Anderson OA, Wearne IM. Informed consent for elective surgery--what is best practice?. J R Soc Med.. 2007; 100:(2)97-100
Association of Anaesthetists of Great Britain and Ireland. Pre-operative assessment and patient preparation: the role of the anaesthetist. AAGBI safety guideline 2. 2010. https://tinyurl.com/yxr2a3o3 (accessed 17 August 2020)
Association of Anaesthetists of Great Britain and Ireland. Checklist for anaesthetic equipment. 2012. https://tinyurl.com/yxhhef7a (accessed 17 August 2020)
Day case and short stay surgery: 2. Anaesthesia.. 2011; 66:(5)417-434 https://doi.org/10.1111/j.1365-2044.2011.06651.x
Cousley A. Documentation of phases of care. In: Cousley A, Martin D (eds). Keswick: M&K Update Ltd; 2016a
Cousley A. The Cousley model. In: Cousley A, Martin D (eds). Keswick: M&K Update Ltd; 2016b
Dunn D. Body art and the perioperative process. AORN J.. 2016; 104:(4)326-340.e4 https://doi.org/10.1016/j.aorn.2016.07.011
Fisher M, Scott M. Patient safety and managing risk in nursing.London: SAGE; 2013
Gray CE, Baruah-Young J, Payne C. Preoperative assessment in patients presenting for elective surgery. Anaesth Intensive Care Med.. 2018; 19:(9)447-452 https://doi.org/10.1016/j.mpaic.2018.06.006
Liddle C. Postoperative care 1: principles of monitoring postoperative patients. Nurs Times. 2013a; 109:(22)22-26
Liddle C. How to reduce the risk of deterioration after surgery. Nurs Times. 2013b; 109:(23)16-17
Martin D. Peri-anaesthesia management of patient care framework. In: Cousley A, Martin D (eds). Keswick: M&K Update Ltd; 2016
National Institute for Health and Care Excellence. Pressure ulcers: prevention and management. Clinical guideline CG179. 2014. https://www.nice.org.uk/guidance/cg179 (accessed 18 August 2020)
National Institute for Health and Care Excellence. Routine preoperative tests for elective surgery. NG45. 2016a. https://www.nice.org.uk/guidance/ng45 (accessed 18 August 2020)
National Institute for Health and Care Excellence. Hypothermia: prevention and management in adults having surgery. CG65. 2016b. https://www.nice.org.uk/guidance/cg65 (accessed 18 August 2020)
National Institute for Health and Care Excellence. Venous thromboembolism in over 16s: reducing the risk of hospital-acquired deep vein thrombosis or pulmonary embolism. NG89. 2019. https://www.nice.org.uk/guidance/ng89 (accessed 18 August 2020)
National Institute for Health and Care Excellence. Surgical site infections: prevention and treatment. NG125. 2020. https://www.nice.org.uk/guidance/ng125 (accessed 26 August 2020)
NHS website. Consent to treatment. 2019. https://www.nhs.uk/conditions/consent-to-treatment (accessed 18 August 2020)
Primiano M, Friend M, McClure C Pressure ulcer prevalence and risk factors during prolonged surgical procedures. AORN J.. 2011; 94:(6)555-566 https://doi.org/10.1016/j.aorn.2011.03.014
Powell R, Scott NW, Manyande A Psychological preparation and postoperative outcomes for adults undergoing surgery under general anaesthesia. Cochrane Database Syst Rev. 2016; https://doi.org/10.1002/14651858.CD008646.pub2
Royal College of Anaesthetists. Chapter 2: Guidelines for the provision of anaesthesia services for preoperative assessment and preparation 2019. (Part of the Guidelines for the provision of anaesthetic services). 2019. https://www.rcoa.ac.uk/gpas/chapter-2 (accessed 18 August 2020)
Royal College of General Practitioners. Quality patient referrals: right service, right time. 2018. https://tinyurl.com/y6b8h9vu (accessed 18 August 2020)
Royal College of Surgeons of England. Commissioning guide: groin hernia. 2013. https://tinyurl.com/y2jhq2ug
Royal College of Surgeons of England. Outpatient clinics: a guide to good practice. 2018. https://www.rcseng.ac.uk/standards-and-research/standards-and-guidance/good-practice-guides/outpatient-clinics/ (accessed 18 August 2020)
Royal College of Surgeons of England. Surgery and the NHS in numbers. 2020. https://tinyurl.com/y262ymx4 (accessed 26 August 2020)
Simpson JC, Moonesinghe SR. Introduction to the postanaesthetic care unit. Perioper Med (Lond).. 2013; 2:(1) https://doi.org/10.1186/2047-0525-2-5
Sundqvist AS, Holmefur M, Nilsson U, Anderzén-Carlsson A. Perioperative patient advocacy: an integrative review. J Perianesth Nurs.. 2016; 31:(5)422-433 https://doi.org/10.1016/j.jopan.2014.12.001
Tang R, Ranmuthugala G, Cunningham F. Surgical safety checklists: a review. ANZ J Surg.. 2014; 84:(3)148-154 https://doi.org/10.1111/ans.12168
Walker IA, Reshamwalla S, Wilson IH. Surgical safety checklists: do they improve outcomes?. Br J Anaesth.. 2012; 109:(1)47-54 https://doi.org/10.1093/bja/aes175
Wicker P. Perioperative practice at a glance, 1st edn. Chichester: Wiley Blackwell; 2015
Wicker P, O'Neill J. Caring for the perioperative patient, 2nd edn. Chichester: Wiley Blackwell; 2010
World Health Organization. WHO guidelines for safe surgery 2009: safe surgery saves lives. 2009a. https://tinyurl.com/t42lk2w (accessed 18 August 2020)
World Health Organization. Implementation manual WHO surgical safety checklist. 2009b. https://www.who.int/patientsafety/safesurgery/checklist_implementation/en/ (accessed 18 August 2020)
World Health Organization. Global guidelines on the prevention of surgical site infection. 2016. https://www.who.int/gpsc/ssi-prevention-guidelines/en/ (accessed 18 August 2020)
World Health Organization. Safe surgery: why is safe surgery important. 2020. https://www.who.int/patientsafety/safesurgery/en/ (accessed 18 August 2020)
Care of the surgical patient: part 1
Matthew Robertson
Graduate Tutor for Operating Department Practice, Northumbria University, Newcastle upon Tyne
View articles · Email Matthew
Claire Ford
Lecturer, Adult Nursing, Northumbria University, Newcastle upon Tyne, explain how to reduce the risk of contamination
View articles · Email Claire
This article provides clinical guidance on the care of a patient undergoing an elective surgical procedure. It discusses preoperative care and the preparation of the patient. It aims to provide an awareness of the complications associated with perioperative care. Through the use of a patient case study, the authors demonstrate the care required across the full perioperative journey from diagnosis to discharge.
Surgery is an inevitable and important part of health care that can offer individuals life-changing interventions for a range of medical conditions ( Wicker, 2015 ). With increased developments in surgical techniques, such as laparoscopic approaches, and innovative strategies delivering better outcomes for surgical patients, surgeries that were once deemed high risk are now considered routine across a wider range of surgical specialties ( Dejong and Earnshaw, 2015 ). As a consequence, the number of surgeries being performed rose by 27% between 2003/2004 and 2013/2014 ( Royal College of Surgeons of England (RCS), 2020 ) and it is now estimated that more than 12 million surgical procedures are carried out in the UK every year ( Abbott et al, 2017 ).
This article aims to provide the reader with clinical guidance for the care of a surgical patient from diagnosis to discharge. It will also examine some of the complications that can occur within the perioperative care continuum (see Glossary for definition of terms) and explore the management strategies that may be used. Because hernia repair has been identified as one of the most common procedures performed in the UK, with over 100 000 of these procedures carried out every year ( RCS, 2013 ), a case study ( Box 1 ) has also been included to help illustrate the care required across the patient journey.
Mr Singh attended his local primary care centre for an appointment with his GP. He was presenting with symptoms of localised discomfort and pain to his left groin and a bulge was visible on standing. The GP assessed Mr Singh and diagnosed him with an inguinal hernia. He explained that he would have to refer Mr Singh to a specialist and his care would involve a surgical procedure performed under general anaesthetic to treat the hernia. The GP, with knowledge of the relevant protocol ( ), was able to refer Mr Singh safely through the appropriate pathway.
Mr Singh received a letter informing him that he was to attend appointments for an outpatient clinic and a preoperative assessment. At the appointment with the operating surgeon (operating clinic), another examination was performed, the required procedure was discussed and after gaining informed consent, arrangements were made for Mr Singh to be listed for an inguinal hernia repair procedure. At the preoperative assessment, He was asked to fill out a basic health questionnaire to assess his past medical history. The information in this would also be used to guide the investigations that need to be carried out. His vital observations were taken by a preoperative assessment nurse to get a baseline reading ( ). Meticillin-resistant swabs were taken to ensure that he was not carrying the antibiotic-resistant bacteria on his skin (had this been the case a treatment package would be given to him to remove the bacteria and reduce his risk of getting an infection or spreading the bacteria). Due to his health and social status he was listed for a day surgical admission.
On the day of the surgery, Mr Singh was welcomed into the day surgery department by a staff nurse, who sat him down in a comfortable chair and was able to reassure Mr Singh about the structure of the day. The nurse then went through a comprehensive preoperative checklist to ensure all the precautionary measures had been taken to ensure patient safety throughout the anaesthetic and surgical phases of care ( ). Mr Singh was asked whether he had showered, was provided with theatre attire, given pre-emptive analgesia and advised of what to expect before and after the procedure.
Mr Singh was collected by a porter from the day surgery admissions unit and taken through to the operating department reception area, where he was met by an anaesthetic operating department practitioner (ODP), who introduced himself and completed the check-in procedure. Mr Singh was settled into the anaesthetic room and reassured before being induced using standard general anaesthesia. His airway was secured using a supraglottic airway device and he was transferred through to the operating room, where he was transferred using a PAT slide and slide sheet on to the operating table. His position was checked, pressure area-relieving devices were put in place, patient warming was attached, and he was made comfortable before the ‘time out’ was performed. Once safe to proceed, the surgical area was cleaned and prepared, sterile drapes applied, and all necessary equipment prepared and surgical instruments and swabs counted.
After successful surgery and completion of the sign-out, Mr Singh was transferred to the post-anaesthetic care unit (PACU) where a specialist practitioner received a full and comprehensive handover from both the anaesthetist and the scrub practitioner. Once Mr Singh was fully awake, aware and his physiological vital signs were within the correct parameters, he was taken back up to the surgical ward to continue his recovery.
The staff nurses on the ward continued to care for Mr Singh and observed him closely for any signs of postoperative complications. His vital observations were taken at required intervals, he was made comfortable, given analgesics and, after a safe period, encouraged to eat, drink and mobilise. Mr Singh was deemed safe to return home the same day and before discharge was provided with detailed information on wound care, medication requirements, advice on recovery and the signs of complications and contact details for any further advice.
Preoperative care
Initial investigation or contact.
Preoperative care starts at the point of diagnosis and referral and is the first opportunity for health professionals to ensure that comprehensive preparation for the surgery begins. This should be from both a physical and psychological perspective because patients should be provided with the opportunity to ask questions about the surgery and aftercare to help reduce any fears and anxieties that they may have (Wicker and O'Neill, 2013). Consequently, primary care staff, including GPs and practice nurses, have a major role to play in the preparation of individuals for surgery, which can positively impact on postoperative outcomes, such as perceived levels of pain and behavioural recovery ( Powell et al, 2016 ). GPs are also responsible for making the initial referral to a surgical specialty and ensuring that comprehensive background information (ie medical history and specific details of the condition) are communicated to the surgical team so that an outpatient consultation clinic appointment can be arranged ( Royal College of General Practitioners, 2018 ).
Outpatient consultation
Delivering a high-quality clinic requires a holistic approach and the most effective and appropriate way to deliver this is to remain focused on the quality of service and ensure that the patient is treated as an individual with particular values, concerns and wishes ( RCS, 2018 ). The surgeon may decide to go through the process of obtaining informed consent at this appointment, which incorporates discussion of the details of the surgical procedure and comprehensive exploration of the risks and benefits of having the procedure; however, the patient must have the capacity to understand the information given and competence to decide on whether to proceed ( Anderson and Wearne, 2007 ). Following the consultation, the surgeon will list the individual for the required surgery and organise a preassessment appointment. In some cases, this could be on the same day, if the service incorporates one-stop clinics, which have been initiated in some areas to help streamline the service and ensure that most of the patient's preoperative care needs are addressed in a single visit ( RCS, 2018 ).
Preoperative assessment
The process of preassessment is essential for identifying any underlying comorbidities that would increase the risk of complications when having a general anaesthetic, as well as anything that may influence the surgical procedure itself ( Gray et al, 2018 ). However, it also provides the ideal opportunity for the early identification of, and attention to, individual patient needs, for patient concerns to be addressed before admission and for patient education about surgical preparation and aftercare ( Association of Anaesthetists of Great Britain and Ireland (AAGBI) 2010 ; AAGBI and British Association of Day Surgery, 2011 ; Wicker, 2015 ; Martin, 2016 ) ( Box 2 ). The investigations conducted at the preoperative assessment would usually include a full blood count (FBC), electrocardiogram (ECG), and lung function tests, but exactly which investigations are needed mainly depends on the level of the surgery (elective surgical procedures are classified as minor, intermediate or major ( Table 1 ), and the comorbidities of the individual ( Table 2 ) ( National Institute for Health and Care Excellence (NICE), 2016a ). The American Society for Anaesthesiologists (ASA) developed a Physical Status Classification System (often referred to as the ASA Grade) ( ASA, 2019 ) which is also used to determine the level of investigations that need to be conducted at the preoperative assessment and communicate patient comorbidities to the anaesthetic and surgical team ( NICE, 2016a ).
;
Grade
Examples
Minor
Excising skin lesionDraining breast abscess
Intermediate
Primary repair of inguinal herniaExcising varicose veins in the legTonsillectomy or adenotonsillectomyKnee arthroscopy
Major or complex
Total abdominal hysterectomyEndoscopic resection of the prostateLumbar discectomyThyroidectomyTotal joint replacementLung operationsColonic resectionRadical neck dissection
ASA 1
A normal healthy patient
ASA 2
A patient with mild systemic disease
ASA 3
A patient with severe systemic disease
ASA 4
A patient with severe systemic disease that is a constant threat to life
ASA 5 (Emergency surgery)
A moribund patient who is not expected to survive without the operation
ASA 6 (Emergency surgery)
A specific situation in which a declared brain-dead patient whose organs are being removed for donor purposes
On the day of surgery, the patient will be visited by a member of the anaesthetic team, either the consultant or a junior doctor, for a variety of assessments to be conducted, ie airway and pain assessment and the risk of developing venous thromboembolism ( ) ( ). A member of the surgical team will also need to mark the site for surgery and complete consent procedures.
;
Surgical site marking is required in an attempt to reduce errors and must be performed only by an appropriate professional, undertaken with an indelible ink pen, using an arrow at or near the intended incision, which must be unambiguous and clearly visible because the site will be checked on three more occasions (leaving the ward, entering the operating department and prior to the incision) ( World Health Organization (WHO), 2009a ). Wherever possible, written consent must also be obtained before the surgery and anaesthetic, which needs to be clearly documented (no abbreviations) and retained in the patient's notes so they can be accessed by all the health professionals ( NHS website, 2019 ).
Nursing and other healthcare staff will care for the patient in the immediate period leading up to the surgery and will ensure that venous thromboembolism prophylaxis, ie antiembolism stockings, are put into place, that preoperative medication (gastric acid suppression and pre-emptive analgesia) is administered, that the patient is showered or bathed and warmed, that protocols have been followed to minimise surgical site infections, jewellery and body piercings have been removed or taped and that the preoperative checklist has been fully completed ( Dunn, 2016 ; WHO, 2016 ; NICE, 2016b ; 2019 ; 2020 ) ( Box 4 ).
; ; ; ;
Glossary of Terms
Day surgery: term used to define the admission of patients to hospital for a planned surgical procedure when they will be returning home on the same day (less than 24 hours)
Inpatient: a person who stays one or more nights in the hospital and receives treatment, lodging, and food
Perioperative: the period around surgery including before, during and after
Preoperative: a period from the time the surgery is scheduled until the time the patient is transported from the ward to the theatre operating table
Intraoperative: the period of care during the operation and ancillary to that operation
Postoperative: the period of care when the patient is returned from the operating department to the ward
Intraoperative care
The safe surgery process continues within the operating theatre and begins with the perioperative team (ie surgeons, anaesthetists, nurses, operating department practitioners (ODPs) and healthcare assistants (HCAs)) discussing the surgical procedures that are listed for the day and any specific patient requirements, eg allergies and equipment requirements ( Wicker, 2015 ). Once the patient arrives at the department a member of the team will admit the patient by checking the surgical safety checklist that was commenced by the staff on the ward, because the ‘check-in’ part of the form must be completed before the induction of anaesthesia ( WHO, 2009a ; 2009b ) ( https://tinyurl.com/yybrj4tl).
This checklist, which can be tailored to the needs of the clinical area, was created to reduce the number of adverse events by improving communication between the perioperative team and, since its introduction, there has been a marked improvement in the quantity of recorded adverse events within the operating theatre ( Walker et al, 2012 ). This is supported by Tang et al (2014) , who found, from their literature review, that effectively implemented surgical safety checklists can help in avoiding complications and reduce postoperative mortality.
The intraoperative process begins with the orientation of the patient to the anaesthetic room, the application of essential monitoring (ECG, pulse oximeter) and the induction of general anaesthetic, using a range of drugs to ensure that the patient is sedated, pain free and, if necessary, paralysed ( AAGBI, 2012 ). On transfer to the operating room, the ‘time out’ element of the surgical safety checklist will be undertaken before the surgical incision in the patient's skin. All members of the team must be present and attentive at this stage because all areas of potential risks are discussed in detail and this is the last opportunity for adaptations to be made to the surgery to prevent unnecessary harm ( WHO, 2009a ). As well as the safe surgical checklist, several considerations also need to be addressed by the perioperative team ( Box 5 ): surgical positioning, skin and nerve damage, patient warming.
Because patients, in most cases, are not able to advocate for themselves, all members of the intraoperative team must ensure that these elements of care are undertaken to reduce harm and achieve high-quality perioperative care ( Cousley, 2016a ). Surgical positioning is of particular importance, not only for ease of surgical access but also to minimise any adverse physiological effects, such as pressure ulcers and nerve damage, which can extend hospitalisation, delay patient recovery and increase costs to the patient and the NHS ( Wicker, 2015 ). These can be avoided with the use of pressure-relieving equipment, use of safe moving and handling techniques and devices, frequent skin assessments and effective communication between the perioperative team ( NICE, 2014 ). The importance of being an advocate for the surgical patient cannot be overstated, especially in an environment as complex as the operating theatre ( Sundqvist et al, 2016 ). The health professional must fully consider any potential risks to the patient and develop a strategy to minimise these risks ( Box 5 ).
Following the completion of the surgical procedure, the intraoperative team undertakes the ‘sign out’, which includes confirmation of the performed surgery, surgical counts of instrumentation, swabs and other supplementary items and any key concerns for recovery or postoperative care ( WHO, 2009a ). These details will be handed over to the post-anaesthetic care unit (PACU) specialist nurse, along with a record of the patient's vital observations while in theatre ( Simpson and Moonesinghe, 2013 ). The PACU practitioner will regularly check the patient's condition, monitor their vital signs, ensure they are comfortable and, if necessary, warmed ( Box 6 ) ( Wicker, 2015 ). They will also pay particular attention to pain relief and the reduction of postoperative nausea and vomiting, which are often the elements of perioperative care that patients most fear before surgery; as a consequence, these must be minimised to increase patient satisfaction but also to promote recovery and reduce the associated postoperative complications ( Liddle, 2013a ).
Postoperative care
Before the patient is transferred back to the ward a comprehensive handover must take place between the PACU nurse and ward staff, including details of the procedure, the patient's condition, level of responsiveness, airway and breathing, oxygen therapy, circulation, wound dressings and drains, fluid output and input, pain levels, medication and any other special instructions ( Liddle, 2013a ; Wicker, 2015 ). As well as the standard nursing roles and responsibilities, nurses caring for surgical patients also need to have a deep understanding of the potential complications that can arise following surgery, such as surgical site infection, pain, hypothermia ( Box 7 ) and how they can minimise risk or recognise early signs of development ( Primiano et al, 2011 ; Liddle, 2013b ; NICE, 2014 ; 2016b ; 2019 ).
Nurses in primary and secondary care are therefore in a unique position and offer a valuable contribution to the care of the surgical patient because they have a major role to play in minimising the risk of harm and ensuring that the patient is returned to normal functioning as soon as possible, depending on the individual's condition and surgical intervention ( Liddle, 2013b ; Cousley, 2016b ).
Due to the high level of iatrogenesis in surgery, patient safety poses a significant problem and almost half of all recorded adverse hospital events are related to surgical care ( WHO, 2020 ). Consequently, because patient safety is ‘at the heart of quality care’ ( Fisher and Scott, 2013: 6 ) it is paramount that health professionals minimise the risk of adverse events occurring by undertaking appropriate risk assessments and effective teamwork ( AAGBI, 2010 ).
For the surgical patient, preoperative care involves preoperative processes and tests and the identification of patient concerns and needs
Intraoperative care should follow a surgical safety checklist. After surgery, particular attention should be paid to preventing postoperative nausea and vomiting, and providing adequate pain relief
In the postoperative period, nurses should be alert to the potential complications that could arise and provide patients with the information they need for discharge
CPD reflective questions
What aspects of surgical preparation do you think are the most important and how can you improve your own practice in relation to preparing patients for their upcoming surgery?
Reflect upon your own practice and consider how postoperative care can be enhanced from the perspective of patient satisfaction and safety
An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
Publications
Account settings
My Bibliography
Collections
Citation manager
Save citation to file
Email citation, add to collections.
Create a new collection
Add to an existing collection
Add to My Bibliography
Your saved search, create a file for external citation management software, your rss feed.
Search in PubMed
Search in NLM Catalog
Add to Search
Care of the surgical patient: part 1
Affiliations.
1 Graduate Tutor ODP, Department of Health and Life Sciences, Northumbria University, Newcastle upon Tyne.
2 Lecturer, Adult Nursing, Department of Health and Life Sciences, Northumbria University, Newcastle upon Tyne.
PMID: 32901557
DOI: 10.12968/bjon.2020.29.16.934
This article provides clinical guidance on the care of a patient undergoing an elective surgical procedure. It discusses preoperative care and the preparation of the patient. It aims to provide an awareness of the complications associated with perioperative care. Through the use of a patient case study, the authors demonstrate the care required across the full perioperative journey from diagnosis to discharge.
Keywords: Care of surgical patients; Patient safety; Perioperative care; Postoperative care; Preoperative care.
PubMed Disclaimer
Similar articles
[Nursing practice of care to patients undergoing elective surgery in the immediate preoperative period]. de Sena AC, do Nascimento ER, Maia AR. de Sena AC, et al. Rev Gaucha Enferm. 2013 Sep;34(3):132-7. doi: 10.1590/s1983-14472013000300017. Rev Gaucha Enferm. 2013. PMID: 24344595 Portuguese.
Perioperative fluid management. Young E, Sherrard-Jacob A, Knapp K, Craddock TS, Kemper C, Falvo R, Hunter S, Everson C, Giarrizzo-Wilson S. Young E, et al. AORN J. 2009 Jan;89(1):167-78; quiz 179-82. doi: 10.1016/j.aorn.2008.12.017. AORN J. 2009. PMID: 19121424 Review.
Care of patients undergoing laparoscopic cholecystectomy. Graham L. Graham L. Nurs Stand. 2008 Oct 22-28;23(7):41-8; quiz 50. doi: 10.7748/ns2008.10.23.7.41.c6711. Nurs Stand. 2008. PMID: 18988582 Review.
Perioperative fasting. Royal College of Nursing. Royal College of Nursing. Paediatr Nurs. 2006 Jul;18(6):33. doi: 10.7748/paed.18.6.33.s27. Paediatr Nurs. 2006. PMID: 16881501 No abstract available.
The PubMed wordmark and PubMed logo are registered trademarks of the U.S. Department of Health and Human Services (HHS). Unauthorized use of these marks is strictly prohibited.
MD | PhD Program
Master's Programs
PhD Programs
Postdoctoral Fellows
Residency & Fellowship
Non-Degree Programs
Visiting Students
Campus Life at U-M
Health & Wellness
Building Your Community
Accessibility & Disability
Departments
Centers & Institutes
Interdisciplinary Programs
Facts & Figures
Medical School Leadership
News & Stories
Requirements
Interview Day
Admissions Chats
AAMC Michigan's 35 Answers
AAMC Michigan's 10 Financial Aid Answers
Admitted Students
Overview & Highlights
Patient Interaction
Chief Concern
Years 3 & 4
Learning Informatics
Training Sites
Leadership Program
Global Health & Disparities
Healthcare Innovation
Health Policy
Medical Humanities
Patient Safety & Quality Improvement
Scientific Discovery
Doctoring Course
Evidence-Based Medicine
Interprofessional Education
DEIAJ Curriculum
Language Opportunities
Curriculum Diagrams
Grading & Assessments
Guideline Budget
Loans & Eligibility
Financial Aid Application Timeline
Scholarships & Grants
Documents & Forms
Tips & Links
Tuition Refund Policies
Consumer Information
Disbursement & Repayment
MD Emergency Student Aid Fund
MD Travel Grant
Child Care Subsidy
Residency Interviewing Loans and Resources
Short-Term University Loan
Contact the Office of Financial Aid
Profiles & Demographics
Culinary Connections
Students with Disabilities
Arts & Humanities
Diversity & Health Equity
Dual Degrees
More Possibilities
Commencement
Available PhD Programs
Academic & Social Events
MSTP Fellows
Application Process
Application Requirements
MD | PhD Curriculum
Undergrad Summer Program
Contact the MD | PhD Program
Bioinformatics
Biological Chemistry
Cancer Biology
Cell & Developmental Biology
Cellular & Molecular Biology
Genetics and Genomics
Health Infrastructures & Learning Systems
Microbiology & Immunology
Molecular, Cellular & Developmental Biology
Molecular & Cellular Pathology
Molecular & Integrative Physiology
Neuroscience
Pharmacology
Recruitment Events
Interview Weekends
Certificates & Dual Degrees
Quantitative & Computational Biology Emphasis
Training Grants
Facilities & Resources
Stipend & Benefits
Professional Development
Finding a Position
Funding Your Postdoc
Hiring Process
Postdoc Preview
International Postdocs
ACGME Fellowships
Non-Accredited Fellowships
Postdoctoral Physician Scientist Training
Salary & Benefits
Prerequisites
Visiting Residents & Fellows
Application Overview & Requirements
Tuition & Fees
Timeline & Curriculum
Information Sessions
Program Details
Undergrad Summer Research
First Days Survival Guide
Health Services
Mental Health
Health, Spirituality & Religion Program
For Partners & Families
Things to Do in Ann Arbor
Getting Around
Graduate Medical Education
Office of Continuing Medical Education
Office of Faculty Affairs & Faculty Development
Office of Graduate & Postdoctoral Studies
Physician Scientist Education & Training
Office of Medical Student Education
Points of Blue
January 30, 2024
Charcot neuroarthropathy (CN), a complication of diabetes-related neuropathy, is a serious condition that can cause significant foot and ankle deformities, chronic ulcers, and even limb loss. The condition often requires large limb salvage reconstructions of the foot and ankle to correct equinovarus deformities, as well as to create a stable, plantigrade foot.
In the case study, Surgical Reconstruction in a Single Patient with Bilateral Avascular Necrosis of the Talus , first author Kanika Kochhar, DPM , along with co-authors Cara Fontana, DPM and Brandon Gumbiner, DPM, highlight the outcomes of a female patient with severe foot and ankle deformity secondary to CN and avascular necrosis (AVN) of the talus to bilateral feet.
The patient underwent two different surgical approaches to correct the foot and ankle deformities. Her right lower extremity was treated surgically with a blade plate, while her left lower extremity was treated with an intramedullary rod. The patient’s presentation was also complicated by Charcot-Marie-Tooth, an inherited disorder of the peripheral nerves, caused by changes or mutations, in a person’s genetic material.
Dr. Kochhar and her colleagues reported that while both limbs have a brace-able functional foot today, a failure in the hardware used in the left limb contributed to the recurrence of her foot deformity and subsequent wound development.
Dr. Kochhar saw this patient when she was a podiatry resident at Katherine Shaw Bethea (KSB) Hospital in Dixon, Illinois. Dr. Kochhar is now a second-year fellow in the Michigan Medicine Podiatry Fellowship Training Program and will graduate in June 2024.
Dr. Kochhar works extensively in the inpatient setting, while also treating patients in the outpatient clinic and Comprehensive Wound Care Clinic . Her research focus is on Charcot neuroarthropathy and related chronic ulcerations, and those at risk for limb loss. She plans to continue pursuing research in these areas in her career.
Paper cited: Surgical Reconstruction in a Single Patient with Bilateral Avascular Necrosis of the Talus . Dr. Kochhar thanks her KSB colleagues, Dr. Cara Fontana and Dr. Brandon Gumbiner, for their work on this publication.
The Michigan Medicine Podiatry Fellowship Training Program provides clinical training in several different areas of related medical specialties, with an emphasis on research and patient populations at risk for limb loss.
We transform lives through bold discovery, compassionate care and innovative education.
Diversity, Equity & Inclusion
Find a Doctor
Conditions & Treatments
Patient & Visitor Guide
Patient Portal
Clinical Trials
Research Labs
Research Centers
Cores and Resources
Programs & Admissions
Our Community
Departments, Centers & Offices
About the Medical School
Global Footer Secondary Navigation
Last updated 27/06/24: Online ordering is currently unavailable due to technical issues. We apologise for any delays responding to customers while we resolve this. For further updates please visit our website: https://www.cambridge.org/news-and-insights/technical-incident
We use cookies to distinguish you from other users and to provide you with a better experience on our websites. Close this message to accept cookies or find out how to manage your cookie settings .
Login Alert
> Case Studies in Adult Intensive Care Medicine
> The Surgical Patient on Critical Care
Book contents
Case Studies in Adult Intensive Care Medicine
Copyright page
Contributors
Levels of Evidence
Abbreviations Referred to in Case Discussions
Chapter 1 Cardiac Arrest: Post Resuscitation Management
Chapter 2 Initial Management of the Polytrauma Patient
Chapter 3 Management of Major Burns on the Intensive Care Unit
Chapter 4 Management of Sepsis
Chapter 5 Rhabdomyolysis
Chapter 6 Management of Acute Liver Failure
Chapter 7 Status Epilepticus
Chapter 8 Acute Ischaemic Stroke
Chapter 9 Subarachnoid Haemorrhage
Chapter 10 Management of Traumatic Brain Injury
Chapter 11 Variceal Haemorrhage
Chapter 12 Surgical Management of Pancreatitis
Chapter 13 Intra-abdominal Hypertension and Abdominal Compartment Syndrome
Chapter 14 Management of the Ventilated Asthmatic Patient
Chapter 15 Pneumonia
Chapter 16 Interstitial Lung Disease
Chapter 17 Chronic Pulmonary Hypertension
Chapter 18 Acute Lung Injury
Chapter 19 The Role of Noninvasive Ventilation Following Extubation of Intensive Care Patients
Chapter 20 Valvular Heart Disease and Endocarditis: Critical Care Management
Chapter 21 Cardiac Failure Management and Mechanical Assist Devices
Chapter 22 Management of Common Overdoses
Chapter 23 Necrotising Soft Tissue Infections in the Intensive Care Unit Setting
Chapter 24 Fungal Infections
Chapter 25 The Acutely Jaundiced Patient
Chapter 26 Massive Haemorrhage
Chapter 27 Glucose Emergencies
Chapter 28 Endocrine Emergencies
Chapter 29 Acid Base Abnormalities
Chapter 30 Nutrition and Refeeding Syndrome
Chapter 31 Pre-eclampsia and Eclampsia in Critical Care
Chapter 32 Airway Management
Chapter 33 Bronchoscopy and Tracheostomy
Chapter 34 Central Venous Catheter Infections
Chapter 35 Ventilator Associated Pneumonia
Chapter 36 Neuromonitoring
Chapter 37 Monitoring Cardiac Output
Chapter 38 The Surgical Patient on Critical Care
Chapter 39 Delirium in the Intensive Care Unit
Chapter 40 Death and Organ Donation
Chapter 41 Managing the Acutely Ill Child Prior to Transfer
Chapter 42 Who to Admit to Critical Care?
Chapter 43 Clearing the Cervical Spine in the Unconscious Patient in the Intensive Care Unit
Chapter 44 Alcohol Related Liver Disease (Whom to Admit to Critical Care, When to Refer to a Specialist Centre)
Chapter 45 Hyperpyrexia
Plate Section (PDF Only)
Chapter 38 - The Surgical Patient on Critical Care
Published online by Cambridge University Press: 04 May 2017
Access options
Save book to kindle.
To save this book to your Kindle, first ensure [email protected] is added to your Approved Personal Document E-mail List under your Personal Document Settings on the Manage Your Content and Devices page of your Amazon account. Then enter the ‘name’ part of your Kindle email address below. Find out more about saving to your Kindle .
Note you can select to save to either the @free.kindle.com or @kindle.com variations. ‘@free.kindle.com’ emails are free but can only be saved to your device when it is connected to wi-fi. ‘@kindle.com’ emails can be delivered even when you are not connected to wi-fi, but note that service fees apply.
Find out more about the Kindle Personal Document Service .
The Surgical Patient on Critical Care
By John Jameson
Edited by Daniele Bryden , Andrew Temple
Book: Case Studies in Adult Intensive Care Medicine
To save content items to your account, please confirm that you agree to abide by our usage policies. If this is the first time you use this feature, you will be asked to authorise Cambridge Core to connect with your account. Find out more about saving content to Dropbox .
Save book to Google Drive
To save content items to your account, please confirm that you agree to abide by our usage policies. If this is the first time you use this feature, you will be asked to authorise Cambridge Core to connect with your account. Find out more about saving content to Google Drive .
Skip to content
State Resources
National Resources
Nursing Organizations
MNWC Initiatives
Maryland Nursing Workforce Center
NextGen NCLEX
Faculty Case Studies
The purpose of this project was to develop a repository of NextGen NCLEX case studies that can be accessed by all faculty members in Maryland.
Detailed information about how faculty members can use these case students is in this PowerPoint document .
The case studies are in a Word document and can be modified by faculty members as they determine.
NOTE: The answers to the questions found in the NextGen NCLEX Test Bank are only available in these faculty case studies. When students take the Test Bank questions, they will not get feedback on correct answers. Students and faculty should review test results and correct answers together.
The case studies are contained in 4 categories: Family (13 case studies), Fundamentals and Mental Health (14 case studies) and Medical Surgical (20 case studies). In addition the folder labeled minireviews contains PowerPoint sessions with combinations of case studies and standalone items.
Lean Management, Patient Safety, Performance Improvement, Quality and Safety
Case study | surgical setup reduction improves patient outcomes.
To be financially viable, a hospital’s operating rooms (ORs) must keep quality and utilization high and expenses low. It’s critical to plan ahead, be prepared, and set volumes correctly. This means an organization’s OR team should be continuously finding ways to improve turnover time in their ORs, while also sustaining improvements to patient safety, staff engagement and organizational costs.
Surgical instrument processing is critical to safe, high-quality surgical care but has receives little attention. Typical hospitals have inventories in the tens of thousands of surgical instruments organized into thousands of instrument sets. The use of these instruments for multiple procedures per day leads to millions of instrument sets being reprocessed yearly in a single hospital. Errors in the processing of sterile instruments may lead to increased operative times and costs, as well as potentially contributing to surgical infections and perioperative morbidity.
When Virginia Mason’s team examined their inventory of surgical instruments they saw, that at any one time, thousands of instruments were being used and processed during setup, surgery, breakdown or sterilization — about 5.2 million instruments per year — and still large amounts of instruments were left unused in storage. Additionally, there were roughly 3,800 unique instruments sets set to different surgeries and different physician’s preferences. Although they had worked hard to keep the inventory down, 3 they knew innovative thinking could help them make lasting improvements.
A quality monitoring approach was developed to identify and categorize errors in sterile instrument processing through use of a Daily Defect Sheet. Virginia Mason Production System ® (VMPS ® ) improvement methods were used to improve the quality of surgical instrument processing through redefining operator roles, alteration of the workspace, mistake-proofing, quality monitoring, staff training, and continuous feedback.
To study the effectiveness of the quality improvement project, a before and after comparison of prospectively collected sterile processing error rates during a 37-month time frame was performed. After implementing a transformation to their operating rooms’ build-to-order (BTO) process, they removed 58,728 unnecessary instruments, and eliminated all $500,000 worth of unused “sleeping” sets — weighing 29,480 pounds — from processing in the first year. In neurosurgery alone, instrument assembly time decreased by 42 percent, and inventory was reduced by 26 percent.
Instrument Assembly Time
Starting with inventory, progressing with data collection
To answer the question of which instruments surgeons needed most or preferred to use, the team examined and collected surgeons’ preferences based on actual usage. The vision, according to the director of sterile processing at the time, was to create a “better patient experience, with fewer defects, faster setup and better patient throughput.”
Team leaders — after evaluating their employees’ interest and aptitude — trained a nominated group of surgical technicians in VMPS ® improvement tools and methods. Following the training, the group took their clipboards, pens and timers to operating rooms, setup areas, breakdown areas, sterilization rooms and storage rooms. They observed the different work areas to understand physician priorities and track how much time was spent on tasks that made a difference to patients and staff versus time spent on wasteful processes that didn’t benefit patients and overburdened staff.
The improvement team was able to easily step into the operating rooms, introduce themselves and explain what type of data they’d be collecting. The work was transparent from the beginning, and no one felt threatened or worried. The surgeons and staff knew they were all a team and that the improvement team was there to improve work for patients and staff alike. They observed each surgeon and procedure five times, building data so that the team could truly understand the current state and begin planning for a better process to test.
Establishing a structure to guide the work
Armed with data, team members came together for a 3P (Production Preparation Process) 4 workshop to set their vision for a dramatically more efficient process. By the end of the 3P, the participants had created a guiding team to determine next steps, oversee all the work and answer any questions that came up throughout the process. The guiding team included a sterile processing leader, operating room leader, improvement office leader, neurosurgeon, surgical technologist, sterile processing technician, project support staff member and administrative support staff member.
Using improvement methods and tools to get results
Next, the team employed the concept of 5S (sort, simplify, sweep, standardize, self-discipline). They discovered that almost 60 percent of the items in their orthopedic case sets were rarely used. This equates to 700 tons of unnecessary instruments being processed, per year. Using data, they sorted which instruments were being used, and simplified the process by removing non-critical instruments left unused. They swept the area by designing a repeatable inspection of case sets, standardized their tray layout, and established a team agreement to continue monitoring.
The creation of the build-to-order instrument sets employed the concept of just-in-time inventory — in which just the right surgical instruments would be delivered just when they were needed — and allowed for customization to each surgeon’s needs for a procedure. The new setup technique made the process of tool assembly much easier for surgical technologists. A production board provided team members with a visual reference of the current demand for supplies.
In an additional improvement event, focusing on the setup for craniotomy procedures, participants discovered how to customize each set, reducing the setup time and the OR space needs in the suite. By the end of the event, they were able to combine sets, reducing their setup time from 34 minutes to 2 1/2 minutes, a 92 percent reduction. The team compared times before and after the improvement events and found that the more limited case sets did not increase overall procedure time but greatly increased OR turnover time.
Seeing financial gains
This work also yields significant financial benefits to a health care organization. A reduction in processing yielded an annual cost savings of $65,000 per year. The number of lost, broken and damaged instruments was also reduced.
Getting results for other surgery sets
The team spread the work by helping other specialty teams, including orthopedics, neurosurgery and thoracic surgery produce similar setup reductions. The results for improving the laminectomy surgical setup were very impressive. After implementing the build-to-order sets, the instrument assembly went from 34 minutes to 20 minutes, 15 seconds. The instrument setup in the OR went from 24 minutes, 9 seconds, to 2 minutes, 29 seconds — a 90 percent decrease. The number of instruments used decreased from 152 to 59, and the number of instrument sets decreased from 5 to 2.
Instrument Assembly
Operating Room Instrument Setup
Number of Instruments
Improving quality and safety
During the assessment of their instrument inventory before the improvement work, the team determined that the large number of unnecessary instruments in storage could have a big impact on safety. Not only was the probability greater for a surgical technologist to select the wrong instrument for a procedure, but the time spent searching for specific instruments and maintaining all these instruments — many of which were processed and sterilized yet never used — could potentially affect patient care.
Before the intervention, instrument processing errors occurred in 3.0 percent of surgical cases, decreasing to 1.5 percent. Improvements were observed in multiple categories of error types, particularly the assembly errors of packaging (from 0.66 to 0.24 errors per hundred cases), and foreign objects (0.17 to 0.02 errors per hundred cases).
Improving patient access and timely care delivery
The lead time for booking orthopedic surgery, for example, went from 65 days down to 21 days. This meant surgeons did not have to wait as long between procedures and could handle an increase in volume of patient cases.
Key takeaway
Surgical instrument processing errors are a barrier to the highest quality and safety in surgical care but are amenable to substantial improvement using improvement techniques.
Originally published May 24 2018, updated July 12 2021
Are you ready to develop advanced process improvement expertise?
Learn more about our virtual intensive certificate program – Advanced Process Improvement Training.
“This course work came in at the perfect time as the topics we covered in class aligned perfectly with a vaccine delivery clinic we created and we used almost every tool taught 100% to deploy something outside of our comfort zone, and it was wildly successful!” – Chuck Hampston, Lean and Process Improvement Coordinator, Memorial Medical Center, Ashland WI
Similar resources
Lean Management, Optimizing Flow, Quality and Safety
Case study | 36-clinic federally qualified health center saves $600k annually improving patient flow.
Case Study | Building a New Outpatient Surgery Center With Patients and Staff in Mind
Podcast | systematizing equity at virginia mason franciscan health, stay connected.
Sign up for our monthly emails to stay up to date with our latest news, resources, case studies, events and more.
Your information will not be shared. Learn more about our privacy policy here .
Complete Your CE
Course case studies, external link, this link leads outside of the netce site to:.
While we have selected sites that we believe offer good, reliable information, we are not responsible for the content provided. Furthermore, these links do not constitute an endorsement of these organizations or their programs by NetCE, and none should be inferred.
Postoperative Complications
Course #30764 - $90 -
#30764: Postoperative Complications
Your certificate(s) of completion have been emailed to
Back to Course Home
Review the course material online or in print.
Complete the course evaluation.
Review your Transcript to view and print your Certificate of Completion. Your date of completion will be the date (Pacific Time) the course was electronically submitted for credit, with no exceptions. Partial credit is not available.
CASE STUDY 1
Patient A is a man 37 years of age who arrives in the PACU following surgical removal of his gallbladder. Surgical intervention using the laparoscopic approach is successful.
Patient A's airway and ability to maintain respiratory stability are evaluated immediately. His respiration is 16 breaths per minute, and his heart rate is 78 beats per minute. Oxygen is being administered at 2 liters via nasal cannula. A pulse oximeter is placed on his left forefinger, and his oxygen saturation is measured at 95%. The patient is arousable but easily drifts off to sleep.
A transfer of care report on the patient is received from the operating room staff. His operative course was unremarkable. Patient history obtained during the preoperative phase of care showed that he was a 2 pack per day smoker, and he denies taking any prescribed or over-the-counter medications. Patient A's weight is documented as 110 kg.
Further assessment of the patient demonstrates normal skin perfusion with good capillary refill in all extremities. He has a drain in his abdomen with a small amount of yellowish discharge. The wound site and sutures are clean and dry without bleeding or discharge. No Foley catheter is in place; when questioned, he denies the need to void. Completing a head-to-toe assessment shows no other alterations from Patient A's baseline.
Patient A wakes when the second set of vital signs is obtained. He reports that his pain is 6 on a 10-point scale. He states that he has pain in his shoulder and pressure in his abdomen. Morphine (5 mg) is ordered for the pain, and 4 mg is administered IV. His wife is in the waiting room, and she comes into the unit to visit and sits by his bed reading while the patient dozes off.
Repeat vital signs are obtained every 15 minutes for the first hour. At 45 minutes after admission, the patient's oxygen saturation is noted to be 90%. PACU staff suction secretions from the patient's throat, and he is instructed on how to use the incentive spirometer. His oxygen flow is increased to 4 liters/minute by nasal cannula. No change in the patient's oxygen saturation is noted over the next 15 minutes despite compliance with the respiratory exercises.
At one hour after admission, the patient's oxygen saturation remains at 89% to 90%, his respiratory rate is 16 breaths per minute, and he is more difficult to arouse. The nurse notifies the physician of the changes in Patient A's status. Oxygen delivery is changed again to a face mask at 4 liters/minute without improvement in the oxygen saturation level. All other parameters remain stable, demonstrating a readiness for discharge.
Despite the improvement in the patient's status, the oxygenation issue remains worrisome. The patient is admitted for an overnight hospital stay, and respiratory exercises are continued, eventually demonstrating an improvement in oxygen saturation to a high of 94%. The next morning, the patient is discharged home.
The assessment of Patient A was thorough and well-organized. The ABCs were evaluated upon admission to ensure the stability of the patient. The history was ascertained, and vital signs were obtained on the recommended basis. However, despite this excellent care, the patient did not demonstrate adequate improvement in his status to be discharged on the same day.
The patient's history of smoking may be the cause of the respiratory insufficiency. Whether the patient was honest in his assessment of his smoking habit could be debated; many patients do not fully and honestly report their cigarette and/or drug and alcohol use. In addition, the patient may not have reported the feelings of nasal congestion and signs of a developing "cold" to the anesthesiologist prior to surgery. Had this been shared, the surgery may have been postponed. The patient may have been instructed to cut back on cigarette use and wait until the cold symptoms subsided prior to having surgery. When patients underreport or are dishonest during the preoperative phase of care, the staff caring for the patient in the postoperative phase is put at a disadvantage.
CASE STUDY 2
Patient B, a woman 31 years of age, is admitted to phase I PACU after undergoing an abdominal hysterectomy. During the preoperative assessment, the patient noted that she is a nonsmoker, has a history of motion sickness, and is quite anxious concerning the surgery and her future prospects, as she will be "sterile" upon recovery. The report from the operating room is that the patient received inhalation anesthesia and a neuromuscular blocking agent during the procedure. Prior to discontinuing the anesthesia, the patient was administered 4 mg of ondansetron for PONV prophylaxis. Also noted was a period of hypotension caused by a significant amount of blood loss requiring the intraoperative infusion of two units of whole blood.
Upon awakening, Patient B is quite agitated. She is moving from side to side and is not yet oriented to place and time. When questioned, Patient B states that her pain is 7 on a scale of 10. The PACU nurse administers 2 mg hydromorphone IV per order. The narcotic appears to begin to take effect, and when questioned, Patient B's pain is now reported as a score of 4. However, she is now complaining of nausea and asking for an emesis basin as she is afraid she will vomit. The nurse asks her to take slow deep breaths through her mouth and encourages her to relax.
When Patient B's complaints of nausea do not recede, the nurse contacts the physician who orders another dose of ondansetron, which is administered. Thirty minutes after medication administration, the patient's complaints of nausea have not subsided and the nurse again requests an order for an antiemetic. At this point, the physician orders a scopolamine patch be placed on the patient. Subsequent to patch placement, Patient B notes that her nausea is resolving.
Case Study Discussion
Preoperative management of Patient B's nausea was handled well. The staff had ascertained the pertinent information; had a risk factor identification scale been utilized, the patient would have been ranked at a very severe level of risk for PONV. The anesthesiologist recognized this risk and treated Patient B with an appropriate dose of antiemetic prior to the termination of surgery.
There were omissions in care that could have reduced the risk of PONV development in this patient. Prior to the first dose of ondansetron in the operating room, a dose of dexamethasone could have been administered to enhance the effectiveness of the serotonin antagonist.
During the PACU phase of care, the nurse caring for Patient B instituted measures to manage both the patient's pain and nausea. However, there were extenuating circumstances that were not considered and could have reduced the development of this complication. It was noted in the operative report that the patient had an episode of hypotension and blood loss; this volume depletion most likely increased the risk of PONV. In addition, the patient may have remained volume-depleted into the PACU, and no note of this was made.
The physician ordered the second PACU dose of ondansetron, which was administered without benefit. The recommendation for rescue management of PONV is to change drug classes if one is not adequate; thus, another drug should have been ordered. The scopolamine patch seemed to have a beneficial response; upon further questioning of the patient, it was discovered that whenever she had previous bouts of motion sickness the patient used patches to help her manage her symptoms. Had this information been ascertained in the preoperative phase, the patch could have been applied preoperatively or in the operating room. It is critical to gather as much information as possible to reduce these types of delays in patient management.
CASE STUDY 3
Patient C is a high school senior. During the opening drive in the Friday night football game, Patient C is hit from behind. When he falls, he sustains open, comminuted fractures of his left tibia and fibula. Because he is unable to stand, an ambulance is brought onto the field to transport the young player to the hospital for evaluation.
Upon arrival at the emergency department, Patient C's leg is examined, x-rayed, and evaluated by the orthopedic surgeon on call. It is determined that prompt stabilization and cleansing of the wound would be optimal for the best possible outcome; thus, Patient C is prepared for surgery. His parents, who were at the game, arrive in the emergency department just moments after the ambulance and are available to give permission for the operative procedure. As Patient C has been medicated for pain, a history is obtained from the parents. There are no notable problems; Patient C is a healthy young man in excellent physical condition. He has not had previous operations and no previous exposure to anesthesia.
Patient C is transferred to the operating room. The anesthesiologist gives the patient a number of preoperative medications, including those to prevent PONV. The anesthesia of choice is enflurane (Ethrane), a volatile gas. The patient first receives succinylcholine prior to intubation, followed by the anesthetic gas. Within minutes, the anesthesiologist notes that Patient C's carbon dioxide levels are beginning to rise. Just as the surgeon is to begin, the patient sustains a cardiac arrest.
The anesthesiologist immediately stops the insufflation of the gas and begins to administer 100% oxygen. A code response is initiated by the remaining members of the operating team. The rescuer performing chest compressions notes that the patient's skin is warm. While resuscitative efforts continue, blood for laboratory evaluation is obtained. The arterial blood gas results demonstrate a pH of 6.9, partial pressure of oxygen (PaO 2 ) of 110 mm Hg, and a partial pressure of carbon dioxide (PaCO 2 ) of 55 mm Hg. At this point, the anesthesiologist's suspicions are confirmed; the patient is experiencing an episode of malignant hyperthermia.
As soon as the diagnosis is confirmed, the staff is ordered to administer dantrolene at a dose of 2 mg/kg. The operating room personnel contact the PACU to ask for assistance in drawing up and preparing the dantrolene. Only one nurse is available to leave the PACU, and she assists with mixing and administering the dantrolene as soon as it is prepared. Additionally, the patient requires repeat doses of sodium bicarbonate to combat the falling serum pH.
Within 15 minutes of administering the dantrolene, the patient begins to demonstrate a perfusing rhythm, although this is punctuated by frequent runs of premature ventricular contractions. Antiarrhythmics are administered to control cardiac complications.
Simultaneously, the patient is cooled with external cold packs applied to the groin and axilla areas. The leg wound is dressed to prevent further contamination during the resuscitative efforts. Repeat blood is obtained for laboratory analysis. The patient's potassium is elevated, and the patient is started on a glucose-insulin drip.
After the patient's cardiac condition is stabilized, the operating room staff request transfer of the patient to the PACU for further management. The patient is moved, and the PACU staff becomes responsible for managing the patient. The antiarrhythmics, the glucose-insulin drip, and the cooling measures are continued. During the first 30 minutes in the PACU, the patient's urine is noted to be a deep red color, indicative of developing rhabdomyolysis and potential renal failure. The patient is given 100 mg furosemide, and fluids are increased to 150 mL/hour. Within 20 minutes, the urine lightens in color, although it retains a reddish tinge.
Approximately three hours after the first cardiac arrest, the patient suffers a second arrest with the development of ventricular fibrillation. A second code response is called, and the patient is again resuscitated with dantrolene, antiarrhythmics, and sodium bicarbonate. Once again, the patient responds to treatment and regains a perfusing cardiac rhythm.
The patient is ordered to receive dantrolene every 4 hours for the following 48 hours to ensure that another episode of malignant hyperthermia does not develop. The patient is subsequently stabilized and transferred to the ICU, where he remains for 72 hours.
Patient C is a perfect candidate for the development of malignant hyperthermia. He is a young male with well-developed musculature. He has had no previous exposure to anesthesia, so his history was not negative for anesthesia complications; it was incomplete. The onset of cardiac arrest was quite rapid in this patient. This devastating complication can be quick in onset, as demonstrated here, or may be delayed and occur later during the operative procedure. The first indication of the development of malignant hyperthermia in this patient was the rising carbon dioxide level. The skin temperature remained normal during the early phase of development; the first person to note the rise in body temperature was the rescuer performing chest compressions.
The patient was managed appropriately. The staff was required to perform a number of actions to save this patient's life. Administering medications, preparing those medications, cooling the patient, and monitoring blood laboratory values is only part of the picture. The additional PACU nurse pulled to the operating room to help with the resuscitation was instrumental in providing the additional hands and expertise needed in this case.
Upon arrival in the PACU, the patient continued to require extensive stabilization measures. The repeat dantrolene had been ordered but had not yet been administered when the patient sustained the second cardiac arrest. It is imperative that the administration of repeat doses of dantrolene be continued to prevent this type of occurrence. Fortunately, the patient was young and healthy and responded to the treatment.
The long-term outcome for this patient was excellent. The resuscitative efforts were exceptional, and the patient did not sustain any long-term neurologic deficits. It is important to point out that the patient did not have his fracture stabilized at this time. Subsequent surgery was delayed to ensure the stability of the patient. Once stable, the patient had the orthopedic repair performed with epidural anesthesia. Although the risk of developing malignant hyperthermia again while undergoing epidural anesthesia is small, dantrolene was used prophylactically to ensure patient stability throughout the procedure.
CASE STUDY 4
Patient D is a male patient, 32 years of age, undergoing an uncomplicated bowel resection to repair damage and scarring of the bowel secondary to a traumatic automobile accident five years prior. The patient is a healthy, active male who states that he has smoked a pack of cigarettes a day off and on for the last 15 years. He had quit smoking after his auto accident but started again three years previously. His history is unremarkable for cardiovascular disease, and his anesthesia provider has reviewed his previous surgeries, performed at the time of the accident.
During surgery, the patient receives general inhalation anesthesia, intravenous narcotics, and neuromuscular blocking agents. The procedure runs approximately four hours in length. During the procedure, the patient has one short episode of hypotension that was managed with volume replacement.
Upon arrival in the PACU, the patient's vital signs are: blood pressure 118/62 mm Hg, pulse 78 beats per minute, respiratory rate 22 breaths per minute with shallow respirations, temperature 36.5°C, and oxygen saturation 91%. The patient had been extubated in the operating room just prior to transfer to the PACU. The nurse caring for the patient notes the signs and symptoms of respiratory distress, including the high respiratory rate, the shallow respirations, and the low oxygen saturation level. When the patient awakens complaining of pain, the nurse is hesitant to give too large of a dose of the narcotic that had been ordered.
After 30 minutes, the patient's respiratory rate is 18 breaths per minute, the oxygen saturation is 93%, and the patient is more alert. However, the patient continues to complain of ongoing pain, and the nurse leaves the patient's bedside to obtain the narcotics. Upon returning to the patient, the nurse finds the patient dozing. When the patient wakes, the nurse asks him to use the incentive spirometer; he had been instructed in its use in the preoperative phase of care. The patient complains of increasing abdominal pain and refuses to use the spirometer. At this point, the nurse chooses to administer 3 mg of hydromorphone as ordered for pain by the surgeon.
After receiving the hydromorphone, the patient again dozes off and appears to be comfortable. When obtaining the next set of vital signs, the nurse notices that the oxygen saturation has again dropped to 91%; however, as the patient's respiratory effort appears to be adequate, the nurse assumes this low saturation is a consequence of his smoking history. The patient has oxygen supplied by nasal prongs, and the nurse chooses not to intervene further. The patient is left sleeping while the nurse assists in the admission of another patient to the PACU.
Forty-five minutes after arrival in the PACU, Patient D experiences a respiratory arrest. The nurses immediately call a code and initiate resuscitative measures. The patient is administered naloxone, and positive pressure ventilation is initiated. However, bagging the patient is extremely difficult; the pop-off valve goes off with each ventilation, and the patient's chest is not rising as hoped.
Fortunately, the anesthesia provider responds and immediately asks for an endotracheal tube to reintubate the patient. When attempting to intubate the patient, the anesthesia provider finds it very difficult as a result of the patient developing laryngospasm. Succinylcholine is administered, and high positive-pressure oxygen is given via a jet vent. After another two attempts, the patient is successfully intubated. The patient is then placed on a mechanical ventilator with positive-end-expiratory pressure applied to help reduce the buildup of fluid in the lungs. He is started on a course of antibiotics and steroids and admitted to the ICU. After two days, the patient is extubated, moved to the surgical floor, and at day 6, is discharged from the hospital.
Patient D is a typical postoperative patient. He was healthy and had an uncomplicated surgical event. He should have progressed through the recovery period without a problem; however, he sustained a respiratory arrest and his recovery was prolonged. Fortunately, he survived without long-term sequelae.
The nurse caring for Patient D made assumptions about his condition based upon his preoperative history. The smoking history allowed her to be lulled into a sense of security knowing that smokers have altered oxygen saturations. His appearance of ease was comforting, and she became complacent in her vigilance.
When Patient D sustained the respiratory arrest, the initial cause was unknown. He had numerous risk factors; the arrest may have been caused by the dose of narcotics, in which case, naloxone would have been a treatment of choice. This was tried but without a successful response. He was hypoxemic upon arrival in the PACU, as evidenced by his low oxygen saturations. This hypoxemic state may have precipitated the respiratory arrest. In addition, he had received neuromuscular blocking agents in the operating room and the arrest may have been secondary to residual paralytic agent. However, upon intubation he was noted to have developed laryngospasm, which may indicate that he sustained an episode of NCPE. He was a candidate for NCPE due to his age, preoperative health status, and early extubation.
Whenever a patient sustains a life-threatening event such as a respiratory arrest, it is critical that care providers work to determine the cause. Identification of the cause can lead to the appropriate choice of a resuscitative effort. In this case, the nurse acted appropriately in administering the naloxone, although it was later determined that this was not the cause of the arrest. Despite the fact that NCPE was not considered until the patient was found to have a laryngospasm, the measures undertaken were appropriate. The only error was the complacency that the nurse exhibited towards the patient's status upon arrival in the PACU and the first 45 minutes of care. Early attention to the hypoxemic state may have prevented the development of the arrest, although this does not always make a difference in cases of NCPE.
Patient D should be educated prior to discharge regarding the development of this side effect. If further surgeries are needed, it is imperative that he be able to relate this information so that measures can be instituted to reduce the risk of respiratory compromise.
CASE STUDY 5
Patient E, a man 74 years of age, is undergoing surgery for a blockage in his left femoral artery. The patient has a history of significant vascular compromise of his left leg secondary to the blockage. A stent is placed during surgery, and the patient is subsequently transferred to the PACU. Upon arrival in the PACU, his vital signs are: blood pressure 162/86 mm Hg, pulse 80 beats per minute, respiratory rate 16 breaths per minute, core temperature 34.5°C, and oxygen saturation 90%. The patient was extubated prior to arrival in the PACU. After the patient is stabilized and an assessment is completed, he is warmed using a warm air convection device. To combat his low oxygen saturations, his oxygen flow is increased to 6 liters per nasal cannula.
Fifteen minutes after arrival, the patient complains of severe pain in his left leg. His peripheral pulses are good, and his color is pink. However, as this was the surgical site, the nurse immediately contacts the surgeon. The surgeon speculates that the pain is secondary to new perfusion in this leg and the removal of sequestered by-products of circulation. He orders the patient to receive 3 mg hydromorphone for pain, which helps resolve the patient's complaints.
One hour after admission, the patient's vital signs return to preoperative values; his body temperature is now 36°C. At this point, he complains of pain in both lower extremities. Upon assessment, it is found that his peripheral pulses are weak in the right leg and the color of this extremity is dusky and cool to touch. His left leg remains warm, pink, and with good peripheral pulses. The patient's legs are elevated on a pillow to improve blood return to the heart, and he is again administered hydromorphone. After the second dose of hydromorphone, the patient drifts off to sleep. When he wakes, he continues to complain of pain in both extremities. The right leg remains cool, dusky, and with poor peripheral perfusion. The nurse again contacts the surgeon, who determines that the patient is possibly developing a DVT in the right calf. The patient has graduated compression stockings applied to the right leg to reduce the risk of further clot formation. As the patient had been heparinized in the operating room, no further anticoagulants are ordered.
The patient is discharged from the PACU to the surgical ward. At day 3, when he is ambulating in the hall, Patient E suffers a cardiac arrest and is not able to be resuscitated. He most likely sustained a pulmonary embolus secondary to the DVT in the right leg. The ambulation may have caused the clot to be knocked loose, allowing it to travel to the pulmonary vasculature.
This patient was at high risk for DVT formation both due to the type and extent of surgery as well as his history of peripheral vascular disease. As he was anticoagulated in the operating room, no further interventions were instituted. However, the guidelines for management and prophylaxis of this type of patient recommend the institution of graduated compression stockings or intermittent pneumatic compression devices in addition to anticoagulation [50] . It can be speculated that this may have reduced his incidence of DVT formation; however, due to his extensive vascular history, he was at high risk prior to, during, and after surgery. It would be speculation to determine if this event may have been preventable.
The nurse caring for the patient performed her job according to policy. The only change that may have been recommended is the placement of the graduated compression stockings on the right leg prior to surgery or after the patient was stabilized in the PACU.
CASE STUDY 6
Patient F, a woman 47 years of age, has sustained a comminuted fracture of her left tibia and fibula after falling on wet grass. Patient F is transferred to the emergency department, where the determination is made to take her to the operating room for internal fixation and subsequent casting.
Following surgery, Patient F is admitted to the PACU with a cast on her left leg. The leg is elevated on top of pillows to ensure adequate drainage. Upon awakening, the patient complains of pain of 9 on a 10-point scale. She is medicated with hydromorphone and falls back to sleep. Forty-five minutes later, she again complains of continued pain. At this point, she receives 3 mg of intravenous morphine. While reviewing the patient's chart and medication orders, the PACU nurse discovers that the patient has a history of frequent narcotic use and is labeled a "complainer" who is frequently seen in the emergency department or physician's office with vague complaints of pain and requests for refills of her narcotics.
After two hours in the PACU, the patient is transferred to the orthopedic floor for continued recovery. Other than her complaints of pain, her PACU stay is uneventful. When giving report to the nurses on the floor, the PACU nurse relays her findings regarding the patient's complaints of pain and repeat requests for pain medications.
During the remainder of the day and into the evening shift, the patient is monitored every four hours. She is medicated as ordered, but within one to two hours after receiving her medications she calls the nurse for additional analgesia. She continues to complain of pain, stating that she feels a burning sensation in her left leg. Her cast is checked and appears to be intact, without peripheral swelling of her leg, and peripheral pulses are present but weak.
At midnight, the patient calls the nurse with continued complaints of pain. The nurse notes that the cast is tight; the patient is no longer keeping it elevated as instructed. The orthopedist on call is contacted, and the decision is made over the telephone to bivalve the patient's cast to ensure adequate circulation. This is accomplished, and the patient appears more comfortable, although her reported pain score remains at 6.
The following morning the patient is seen by the orthopedic surgeon, who notes the bivalved cast and continued complaints of pain. The surgeon orders the cast to be replaced, which is accomplished. That evening the patient again complains of pain, this time giving a score report of 10. The physician is again contacted by telephone, and additional pain medications are ordered. Throughout the night, the patient continues to complain of pain despite frequent doses of narcotics.
The patient is scheduled for discharge in the morning. When seen by the surgeon prior to discharge, it is noted that the patient's foot is cool to touch and peripheral pulses remain weak. She has continued complaints of pain and does not want to be discharged at this time. At this point, the surgeon considers the possibility that the patient may be developing a case of compartment syndrome. The cast is removed, and the extremity is tense and cool, with poor color. The patient is immediately taken to the operating room, where a fasciotomy was performed. Upon opening the compartment, it is noted that there is extensive necrotic tissue that requires debridement. The remaining amount of muscle is minimal. The patient eventually recovers but with severe disability in her ambulatory capabilities.
This patient sustained a long-term disability secondary to rapidly developing compartment syndrome. As discussed, rapid assessment and intervention is required to prevent this type of sequelae. The classic sign of compartment syndrome is pain that is out of proportion to the injury. This patient had continued complaints of pain; however, due to her history as someone who was always complaining of pain, her complaints were not taken seriously. All patient complaints should be addressed and believed; the lack of attention to these complaints led to a long-term disability in this patient.
Compartment syndrome is a common complication following fracture, and the possibility of this complication should have been recognized earlier. In fact, the first evening, when the first cast was bivalved, compartment syndrome should have been considered. It was more than 36 hours before the diagnosis of compartment syndrome was made, enough time for severe tissue necrosis to develop. Had the patient undergone a fasciotomy rather than bivalving the cast, the outcome may have been different.
This case demonstrates the need for prompt recognition of patient's complaints and consideration of all potential complications, regardless of the patient's previous history. The nurses and physicians in this case neglected the patient's pain complaints because of her prior history. The patient should have been given the benefit of the doubt, which may have allowed for earlier intervention.
This case subsequently went to litigation. The physicians involved in her care admitted to malpractice in neglecting to recognize and diagnose the development of the compartment syndrome earlier in her care when the potential for complications may have been decreased. The nurses admitted to malpractice as they chose to disregard the patient's complaints when further investigation should have been undertaken. It is a sad outcome, especially as it was a preventable complication.
CASE STUDY 7
Patient G is a man, 83 years of age, who is undergoing colon resection for removal of cancerous nodes. The operative procedure proceeds without complication, and the patient is transferred to the PACU without incident.
During the first postoperative hour, the patient is noted to be hypotensive, with a systolic blood pressure of 80 mm Hg. A review of the patient's history indicates that his normal systolic pressure on admission was 160 mm Hg. The patient is noted to take furosemide, hydrochloride thiazide, metoprolol, and lisinopril for blood pressure control. With this information in mind, it is obvious that the patient's systolic pressure is significantly lower than anticipated.
Upon awakening, the patient is confused and disoriented. He needs continual reminders to help orient to person, place, and time. He is not compliant with postoperative instructions and tries to remove the dressing from his abdomen. He complains of pain when asked but is not able to rate the pain on a scale of 1 to 10. He requires wrist restraints to prevent him from disrupting the surgical site.
The patient is also noted to have a history of congestive heart failure following a myocardial infarction many years ago. While fluid resuscitation would be the first step in supporting the patient's blood pressure, the risk of developing further cardiac failure should be considered. Prior to instituting further management, the patient's history and medication use is reviewed.
The patient stated upon admission that he had been NPO after midnight, as instructed. He was told to take his medications in the morning with a small sip of water prior to arriving at the hospital, to which he complied. His wife told the nurses that he did not eat the food recommended on his bowel prep program the evening before surgery; he was anxious and wanted to ensure that his colon had been cleaned out sufficiently. His wife also noted that he had complied with the bowel prep cleansing as instructed.
The patient is administered additional intravenous fluids at a rate of 75 mL/hour. He is finally discharged from the PACU five hours after surgery and transferred to the surgical ward. On the surgical ward, his blood pressure remains low, with an average systolic pressure of 90–100 mm Hg. The patient is discharged on day 3 with a blood pressure of 102/86 mm Hg.
This case presents the typical complication of under-resuscitation and subsequent volume depletion. The patient's response to this complication was the development of a prolonged hypotensive episode, complicated by confusion and disorientation upon awakening.
Further history should have been ascertained from the patient and the patient's wife prior to surgery. The staff was unaware that the patient had been NPO for such a length of time. When asked if he complied with the bowel cleansing as ordered, the patient replied yes; no further questions were asked to ensure how he complied, when he last ate, etc. This assumption increased the risk of compromise.
In addition, the patient took his normal blood pressure control medications prior to surgery. While holding of these medications is often done on the day of surgery, the nurses needed to recognize the potential risk this offered. Ensuring adequate resuscitation and volume status in the preoperative and operative phases of care should have been instituted.
Anesthetic agents are vasodilators. This combined with the administration of blood pressure reducing agents caused a significant drop in the patient's systolic pressure. The patient's systolic pressure remained low even at the time of discharge; it is critical to alert this patient to this development and ensure that the patient follow up with either the surgeon or the cardiologist. As the drugs cleared from the patient's body, the normal systolic pressure should have been achieved.
The confusion and disorientation that developed in the PACU was most likely a consequence of low perfusion pressure within the cranial cavity of this patient. There are several reasons for postoperative confusion in the elderly; those reasons should be identified and treated. In this case, had the patient received fluid resuscitation earlier in the course of care, this neurologic development may have been avoided.
Managing an elderly patient with a history of multiple disease processes, medication use, and anesthetic administration is challenging. Further in-depth evaluation and history taking is critical to ensure safe care delivery throughout the operative period.
CASE STUDY 8
Patient H, a man 34 years of age, is admitted to the PACU following abdominal surgery for colitis. In the operating room, the patient's disease was found to be extensive, and he now has an ileostomy for stool drainage. He had a large mid-line incision reaching from the pubis to the distal sternum.
Upon admission, his vital signs are: blood pressure 102/60 mm Hg, pulse 72 beats per minute, respiratory rate 16 breaths per minute, oxygen saturation 94%, and core temperature 35°C. He is somnolent but opens his eyes upon repeated commands. The formation of the stoma was discussed with the patient prior to surgery as a last choice option; however, he was unaware at that point in his care of the extent of his disease and the need for the ileostomy.
After 15 minutes, the repeat vital signs are unchanged except for the blood pressure, which is 90/58 mm Hg. His body temperature remains at 35°C. Measures to rewarm the patient are undertaken. He continues to sleep, although he is arousable. After 30 minutes, the patient's blood pressure drops to 84/48 mm Hg. It is also noted that urine output is only 5–10 mL of dark yellow urine in the Foley catheter tubing. The physician is notified, and she orders a fluid challenge of 100 mL.
After the fluid challenge, the patient's blood pressure rises to 92/60 mm Hg. Although this is below baseline, it does show improvement. However, urine output remains the same; there is no recognizable response to this fluid challenge. The ostomy drainage does increase and is measured at 100 mL of very light yellow liquid.
Two hours after admission, the patient remains in the PACU. His core body temperature remains low, and his blood pressure is below baseline. Little urine output has been noted, but ostomy output is at 250 mL since surgery. Bowel tones are heard as high-pitched squeaks. Additionally, the patient remains significantly sleepy and slow to respond to commands.
After three hours, the patient is transferred to the surgical inpatient unit. His blood pressure is 98/60 mm Hg, pulse 70 beats per minute, respiratory rate 16 breaths per minute, core body temperature 35°C, and oxygen saturation 96%. Urine output totals 30 mL since the end of surgery; ostomy drainage totals 350 mL. The patient is arousable but sleeping when not stimulated.
That same evening, approximately seven hours after surgery, the patient is awake and complaining of severe abdominal pain. His abdomen is distended; ostomy drainage now measures an additional 300 mL, and urine output is 150 mL. The surgeon is notified, and the patient is evaluated. At this point, the surgeon speculates that there may be leakage at the stoma site. The patient is prepped for the operating room for further evaluation.
While waiting for the surgical team to arrive, the patient begins passing a significant amount of gas into the ostomy bag. The amount of drainage remains high, but with the passing of the gas the distension begins to resolve and the patient notes that his pain has diminished. It is determined that the surgery will be delayed pending resolution of the abdominal distension.
The patient remains in the hospital for another four days. He receives instructions on how to manage his stoma and ostomy. His stoma drainage remains high for the first two days. He tries solid foods on day 3 but develops severe abdominal cramping and distension yet again. His diet is changed to soft foods, and over the course of the next week, he is eventually able to tolerate a normal diet.
This patient was admitted following an extensive abdominal procedure. Upon arrival in the PACU, his core body temperature was low; however, this is common in patients undergoing an open abdominal procedure of extended length. The only error in care was the delay in beginning to warm the patient. Rewarming measures, using forced air warming, should be the standard of practice for this type of patient.
The patient developed hypovolemia, as evidenced by his low blood pressure. This period of decreased circulating volume could have potentiated the risk of subsequent ileus formation. The fluid challenge of 100 mL was ordered without awareness of the ostomy output. This output should be included in the volume assessment of the patient prior to reporting his vital signs. Most likely, a large fluid challenge would have benefited the patient and could have helped to prevent the ileus formation.
When the patient complained of severe pain while in the nursing unit, it was appropriate to consider the risk of failure of the stoma sutures. This is not an uncommon complication in this type of surgery, especially with the distended abdomen. However, the patient required a more detailed evaluation prior to being prepped for surgery. Ileus formation was not considered because the patient had audible bowel tones. While most patients with postoperative ileus do not exhibit bowel tones, these tones are not uncommon for patients with a stoma and significant changes in their GI tract. One procedure that may be beneficial for these patients is the insertion of a tube into the stoma. However, with the concern of disruption of the sutures, this was not an appropriate course of action for Patient H and was not performed.
While the patient did exhibit postoperative complications, the development was not unexpected. The assessment of the patient could have been better; assessing the intake and output beginning before surgery may have alerted the staff to the hypovolemic state. If this had been recognized and treated earlier, the ileus formation may have been averted. However, it is not uncommon for this patient type to develop an ileus, so it is difficult to determine whether it was a controllable complication. The patient's ultimate outcome was not affected by these complications, but his recovery period could have been more comfortable and without risk had certain assessment parameters been monitored more closely.
CASE STUDY 9
Patient I is a girl, 5 years of age, undergoing a surgical intervention to correct a congenital cleft lip and palate. She is small for her age and has had multiple difficulties with food intake. During the first year of life, it was nearly impossible for her to suck either at the nipple or on a bottle due to the shape and size of the defect. Despite multiple attempts and alternative methods of feeding, her growth has been slowed due to malnourishment. As she became able to ingest solid foods, she had difficulty with swallowing and had multiple bouts of sinus infections due to food particles being forced into the open sinuses.
In the preoperative phase of care, Patient I is noted to be quite anxious, crying in her mother's arms and shying away from the caregivers. She does not want an IV line started and throws a tantrum when this is attempted. Despite her young age, she is well aware of the multitude of interventions that occur in a hospital setting and she is determined to maintain some control over these developments. Her mother comforts her and does not appear to have much control over Patient I's behavior.
The corrective repair progresses without complication, although the surgery is long, more than six hours in length. When Patient I is transferred to the PACU, she is intubated and asleep. The surgeons do not want her to awaken abruptly and risk dislodgement of the endotracheal tube and/or damage to the surgical site. Her vital signs are stable compared to those obtained during the preoperative phase of care. She has an IV line in her right forearm, a Foley catheter, and cardiac monitoring electrodes on her chest, along with the endotracheal tube.
After Patient I is stabilized in the PACU, her mother is allowed in to see her and sit at the bedside. The mother is instructed to watch the patient and notify the nurses if she starts to awaken and reach for the tubes. The mother is overwhelmed by the change in her daughter's appearance, something she has dreamed about for the last five years.
After 30 minutes in the PACU, Patient I begins to move in bed. Her eyes remain closed but she appears to be awakening and somewhat agitated. The orders are to administer narcotics to the patient for pain; however, the patient is unable to use any type of pain scale due to the decrease in cognition. The mother is holding the child's hand when the child pulls her hand away and starts to reach for her mouth. The nurse sees this happening and is able to grasp the child's wrist and prevent her from reaching the tube and surgical site. Wrist restraints are applied to ensure that the patient is not able to repeat this potentially life-threatening action.
At 60 minutes, the patient begins to open her eyes and starts to move from side to side. She is pulling against the restraints and trying to sit up so she can reach the endotracheal tube to remove it. The nurse instructs the patient that she must lie still and that the tube must remain in place. The nurse attempts to use an illustrated pain scale, but the patient refuses to cooperate, continuing to pull at the restraints.
During this combative period, the patient's blood pressure and pulse rate continue to rise and blood is noted on the dressing around her mouth. It is imperative that something be done to reduce the risk of damage; the nurse decides to medicate the patient with the narcotic ordered to help control the agitation and allow the child to relax and perhaps fall asleep. This objective is achieved, and the patient falls asleep and appears relaxed. Her vital signs again return to preoperative values.
Ninety minutes after surgery, the surgeon enters the PACU to examine the patient. While touching the patient's dressing, the patient's eyes open; she grasps the hand of the surgeon and tries to grasp the endotracheal tube. She is shaking her head violently from side to side, and the dressing on her face begins to loosen. The physician yells for assistance, and the nurse holds the head of the child still so the tube and dressing can be re-stabilized and secured. The look in the eyes of the child is one of pure terror. By now the only way the patient is able to lash out is to kick her legs, and she is thrashing about in the bed. Her mother is trying to calm her, but the child does not appear to recognize her mother or at least does not respond to the mother's efforts.
The surgeon orders a dose of midazolam in an effort to calm the child and ensure the safety of the tube and surgical site. After administration, the child does calm down and is no longer struggling; however, she does not appear to fall asleep. She continues to have a very scared look in her eyes, and she does not appear to be fully aware of what is going on around her. Within 20 minutes, the child is dozing quietly and appears to be much more comfortable.
Two hours after surgery, the patient again awakens and is calm and cooperative. She is responding to her mother and is receiving comfort from her mother's presence. She is again instructed as to the need for the restraints and is not pulling against them. She tries to talk and begins coughing against the endotracheal tube. The surgeon has ordered that the patient remain intubated for at least the first 48 hours post-surgery to ensure adequate time for the wound healing to begin. This is going to be a challenge with this patient as she is trying continually to either remove or talk around the tube.
The patient is stable at three hours and is transferred to the ICU, as she remains intubated. Report is given to the staff. While the patient is being moved to the ICU bed and her hands are free, she grabs the endotracheal tube and pulls. Fortunately, she is prevented from removing the tube, although the tube is checked to ensure proper placement. At 48 hours, she is extubated and transferred to the pediatric floor. Within four days she is discharged home without further complication.
This child presents a number of challenges to the PACU staff. Airway management is always the first step in stabilizing a patient who has arrived from the operating suite, and this patient did have a secure airway at the time of transfer. The concern developed when the patient began to awaken and tried to remove the tube. Had she been successful at pulling the tube, this could have been a life-threatening complication. Attempting to mask ventilate the child would be challenging with the surgical repair site preventing the achievement of a good seal with the mask. Re-intubation would have to be performed with extreme caution to prevent damage to the surgical repair.
The child was initially stable, and the recovery appeared to be without incident. However, after the child started to awaken she demonstrated many of the signs of emergence delirium, which is more common in children than adults. She was thrashing about, pulling on her restraints, and uncooperative with instructions. Her mother did not appear to be able to calm her, indicating the possibility that she was disoriented and confused.
While the nurse was aware of the need to protect the child, she chose to administer the narcotics as ordered rather than receive an order for a different medication. It may have been that the narcotic was the right choice; the patient could have been in pain, although this was not assessed due to her behavior. On the other hand, the narcotic could have caused the second bout of combativeness noted upon the surgeon's arrival. When the patient was able to grasp the endotracheal tube, it was determined that the mother had released the restraint while holding her daughter's hand. This could have been another life-threatening complication; the nurse needed to not only ensure that the mother understood the need for the restraints but also check for proper placement of the restraints when her vital signs were obtained.
Midazolam was the drug that was able to allow the child to fall asleep and awaken in a more controlled state. Although midazolam may be a cause of emergence delirium and confusion in children, it is also one of the first drugs considered in its management. For this patient, it was the right drug, although the right time may have been during the first episode of combativeness. Not all children must be medicated; however, with the risks of tube dislodgement and surgical site disruption being quite high in this child, the administration of midazolam in the earlier phase of care may have been a better choice.
This case demonstrates the multitude of issues in dealing with pediatric patients. Although patients are educated prior to the surgical intervention, this education is not fully understood and the child may not follow instructions as directed. The mother was an excellent source of comfort to her child but also put her child at huge risk by untying the restraints. Parents should have continual reminders of their place in the care of their child.
The risk of postextubation croup was not addressed but could have presented a significant challenge to this patient either in the ICU or once on the pediatric unit. The risk of this form of croup increases when the patient has remained intubated for a length of time and/or when the child fights against the tube, both risk factors in this case. Fortunately, this did not occur and the patient was eventually discharged without further incident.
Children present challenges regularly in the PACU. Their risk of compromise is greater, and the complications are different. Astute care will allow for safe recovery during this period.
CASE STUDY 10
Patient J is a man, 87 years of age, undergoing surgical repair of a fractured hip. He was living at home independently when he slipped and fell in the bathroom, fracturing his right femoral neck. He was on the floor for an indeterminate amount of time prior to being found by a neighbor who checked on him when he had not been seen for a number of hours. Emergency service personnel were called. They found the patient on the bathroom floor in a confused state. He was unable to accurately note the date or time, and he had no recollection of how he ended up on the floor. During the head-to-toe assessment, it was noted that Patient J had sustained a small scalp laceration over his right temporal region, which was clotted by the time the ambulance personnel arrived. His leg was in a displaced position, and a fractured hip was suspected. He was also noted to have a healed scar on his sternum, indicative of a previous open-heart procedure.
Upon arrival in the emergency department, the patient is evaluated by orthopedic, cardiology, and neurology specialists. His history is reviewed and reveals a previous open-heart procedure eight years prior to admission, a long history of smoking prior to the cardiac procedure, and a history of lifelong obesity. The patient's skin condition is poor; he has multiple bruises in varying stages of healing. He has multiple folds of fatty skin, and between these folds, the skin is quite dirty and foul smelling, indicating a poor hygienic state. He has a list of medications in his wallet, which identifies the following drugs: digoxin, simvastatin, furosemide, potassium chloride, amlodipine, and lisinopril. Due to his current state of confusion, the accuracy of this list and the last time the patient took his prescribed medications are unable to be determined.
Patient J's greatest immediate need is stabilization of the fractured femur. The neurologist deems that it is appropriate to perform the surgery under general anesthesia and that postoperative neurologic assessment should be initiated. The cardiologist agrees that the patient is stable from a cardiac standpoint and that he will most likely be able to tolerate the effects of anesthesia. The orthopedic surgeon performs the fractured hip repair.
Upon transfer to the PACU, the patient is still asleep; he was extubated in the operating room, has a cardiac monitor on and a Foley catheter in place, and his hip is positioned for optimum healing. His vital signs are: blood pressure 162/100 mm Hg, pulse 80 beats per minute, respiratory rate 22 breaths per minute, oxygen saturation 89% on 4 liters nasal prongs, and core temperature 34.5°C. No urine is noted in the Foley catheter. The greatest initial concern is the lower oxygen saturation; the nasal prongs are replaced by a face mask at a flow rate of 6 liters per minute. Within 15 minutes of switching the oxygen delivery device, the oxygen saturation increases to 91%.
Thirty minutes after arrival in the PACU, the patient remains asleep. His vital signs are stable; however, his body temperature remains at 35°C despite forced air warming. He is not moving nor does he appear to be in any discomfort. His skin condition does not appear to have improved. His lower extremities are cool to touch, and peripheral perfusion is poor.
At approximately 40 minutes after arrival in the PACU, the patient sustains a cardiac arrest. Resuscitation efforts continue for approximately 20 minutes without success, and the physician in charge pronounces the patient dead.
This patient is representative of the typical postoperative geriatric patient. He has multiple health issues and takes many medications. His physical status is compromised by his nutritional status, in this case, obesity. He was living independently prior to this event; he did not have family close by, and his history was only ascertained by the information that his neighbor and the first care responders were able to locate. Even with that, the accuracy of this information was questioned. Prior to the fall, the patient had been happily living his life, which was subsequently lost after the surgery.
After the patient was pronounced dead, it was speculated that he had developed a clot that occluded his pulmonary vasculature. If this was indeed the case, the outcome would not have changed despite the resuscitation efforts. However, due to his advanced age and condition, a postmortem exam was not performed and the cause of death was never confirmed.
The patient's condition was compromised by numerous factors. He had a positive cardiac and smoking history and may have sustained a neurologic event at the time of the fall, or a neurologic event may have precipitated the fall. His obesity presented a number of issues. His skin condition was quite poor, and his apparent lack of hygiene would increase his risk of postoperative infection. While he was considered to be independent, his current health state was definitely not optimal.
Had this patient survived, in all likelihood, he would not have been able to return to an independent living environment. He would have required care in a rehabilitation facility to learn to ambulate post-surgery. Whether he would be strong enough to recover to a fully independent state was questionable.
This case demonstrates the many issues and challenges in managing the elderly patient. The lack of concrete information in the preoperative stage can impact the decisions that are made in the operating suite. Patient J's poor health status put him at increased risk for complication development. Even if the patient had survived, his long-term outcome would have been significantly different than the lifestyle he had prior to the injury. Preparing the patient and family for these less-than-optimum outcomes should be considered part of the preoperative care measures.
CASE STUDY 11
Patient K is a woman, 42 years of age, who weighs 432 pounds. She has a BMI of 62 and is scheduled to undergo a restrictive bariatric procedure. Her history is positive for hypertension, diabetes controlled with two to three insulin injections daily, gastroesophageal reflux disease, and obstructive sleep apnea. She is nervous prior to surgery, yet anxiously awaiting the new life that she sees in her future.
The operative course of care is unremarkable. The patient has a gastric band placed, creating a small pouch. She is transferred to the PACU having been extubated. Her vital signs upon admission are: blood pressure 182/112 mm Hg, pulse 82 beats per minute, respiratory rate 24 breaths per minute, core temperature 35°C, and oxygen saturation 91%. She remains very somnolent but opens her eyes with loud verbal stimulus.
Upon admission, the concern for this patient is the low oxygen saturation. She maintained a saturation of 94% during the procedure but the postoperative saturation remains 90% to 91%. Oxygen is being delivered by nasal cannula at 4 liters/minute. The nurse caring for the patient is unsuccessful at awakening her for more than a few seconds. The oxygen delivery system is changed to a face mask with a liter flow of 6 liters/minute. Little improvement in the patient's status is seen with this change.
It would be optimal to awaken the patient to have her participate in respiratory exercises; however, she remains quite sleepy while in the unit. Elevating the head of the bed may help her oxygenation but does little to increase her oxygen saturation values. Arterial blood gas analysis is obtained; the results are pH of 7.34, PaO 2 of 74, and PaCO 2 of 47. With these results it is obvious that the patient is hypoventilating, most likely secondary to pressure on the diaphragm limiting her respiratory excursion effort.
The patient remains somnolent for the next four hours. Her oxygen saturation values remain around 91% despite the efforts of the staff. After four hours in the PACU, she is transferred to the inpatient unit for an overnight stay. She remains hypoxic until the following afternoon.
The patient in this case study demonstrated one of the more common complications following bariatric surgery: hypoventilation. The upward displacement of Patient K's diaphragm prevented full expansion of her lungs, causing carbon dioxide levels to rise while oxygenation values remained low. Although the levels were low, they were not to the point of being life-threatening.
One measure that may be used to improve oxygenation in patients following surgery is respiratory exercises to help expand the lungs and encourage the patient to expel secretions. To accomplish this goal, the patient should be cooperative and have an appropriate cognitive level to follow the commands. As this patient remained somnolent for a lengthy period, efforts at obtaining her cooperation were unsuccessful. It is not uncommon for obese patients to experience a delay in awakening following anesthesia. The drugs are absorbed into the fatty tissue, and release occurs over an extended period. One measure that may have been successful in arousing the patient more quickly is a fluid challenge. This extra fluid can often help circulate the remaining anesthetic and speed the metabolism of the medication, allowing the patient to awaken more quickly. While this may not always be the answer to delayed awakening, it is often successful in obese patients.
Fortunately, this patient did not experience any of the other postoperative complications that are common following bariatric surgery. After her respiratory status improved, she was able to meet the criteria for discharge and was sent home the next day.
In follow-up with this patient, she lost more than 100 pounds in the first year following surgery. She started an exercise regimen and is determined to continue with her weight loss. While 100 pounds is quite a bit of weight to lose, her weight is now 330 pounds; therefore, she remains at risk for the complications of obesity. Her diabetes has not resolved, yet she remains hopeful that with continued weight loss, she will one day be free of insulin injections. Morbidly obese patients have a long and often arduous path ahead of them and should not expect miracles to happen overnight.
Hepatopancreatoduodenectomy with delayed division of the pancreatic parenchyma when utilizing a right lateral approach to the superior mesenteric artery
Hepatopancreatoduodenectomy (HPD) is a high-risk surgical procedure. Delayed division of the pancreatic parenchyma (DDPP) was reported as a novel technique in HPD for reducing postoperative pancreatic fistula....
View Full Text
Visualization of cecal tumor by near-infrared laparoscopy and intraoperative colonoscopy
In laparoscopic colorectal surgery, accurate localization of a tumor is essential for ensuring an adequate ablative margin. Therefore, a new method, near-infrared laparoscopy combined with intraoperative colon...
Laparoscopic redo surgery for sigmoid volvulus following laparoscopic sigmoidectomy
Sigmoid volvulus (SV) is an acute abdominal condition characterized by torsion of the sigmoid colon around the mesentery, and often results in intestinal obstruction that may progress to bowel ischemia, necros...
Laparoscopic liver resection for a patient of hepatocellular carcinoma with von Willebrand disease: a case report
The safety of laparoscopic hepatectomy for inherited coagulation disorders is unclear; however, the safety of open hepatectomy has been reported in several studies. Herein, we report the first case of a laparo...
Correction: Laparoscopic repair of a primary parahiatal hernia combined with gastric volvulus: a case report and literature review
The original article was published in Surgical Case Reports 2024 10 :135
A case of chronic expanding hematoma mimicking a cystic pancreatic tumor
A chronic expanding hematoma is an uncommon entity described as an organized blood collection that increases in size after the initial hemorrhagic event without histological neoplastic features. The standard t...
Surgical treatment of appendiceal mucormycosis in an immunocompromised patient: a case report
Gastrointestinal mucormycosis is a rapidly progressing and often fatal disease, predominantly affecting immunocompromised patients. Surgical intervention, in addition to antifungal therapy, is essential. Herei...
A case of successful management for spontaneous rupture of paraganglioma treated with preoperative transcatheter arterial embolization
Tumors arising from catecholamine-producing chromophil cells in paraganglia are termed paragangliomas (PGLs), which biologically resemble pheochromocytomas (PCCs) that arise from the adrenal glands. Spontaneou...
Intestinal obstruction secondary to perforation of Meckel’s diverticulum caused by dentures: a case report and review of literature
Meckel’s diverticulum (MD) is the most common congenital abnormality of the gastrointestinal tract. However, MD is rare in clinical practice, and perforation of a MD by a foreign body is even rarer. Preoperati...
A case of endoscopic submucosal dissection of esophageal acantholytic Paget’s disease with discontinuously spreading and unclear neoplastic extension
Paget's disease (PD) is a carcinoma, in which irregular atypical cells with abundant cytoplasm proliferate mainly within the epithelium and is classified into PD occurring in the breast and extramammary Paget'...
An incidentally found mass on the remnant stomach after a Roux-en-Y gastric bypass
Incidentally found masses are a widely discussed area of medicine, and there are conflicting opinions as to how to deal with these findings, particularly in the stomach—which has limited documentation in the l...
Recanalization of port-superior mesenteric vein thrombosis with long-term anticoagulant therapy after failed early anticoagulant therapy
Anticoagulant therapy with heparin is the first-line treatment for acute mesenteric vein thrombosis and is effective in improving outcomes. Conversely, patients with failed early anticoagulant therapy occasion...
Salvage surgery following tyrosine kinase inhibitor treatment for advanced non-small cell lung cancer
No standard therapy for non-small lung cancer patients that have acquired resistance to tyrosine kinase inhibitor (TKI) therapy has been established. Some can be effectively treated by salvage surgery, though ...
Ovarian endometrioma: a report of a pediatric case diagnosed prior to menstruation
Ovarian endometriomas (OEs) are rarely found in the pediatric population, especially before menstruation. We report a 6-year-old girl who was postoperatively diagnosed with OE before menstruation.
Gerbode defect resulting from Group B Streptococcus infective endocarditis: a case report
Gerbode defect is an unusual abnormal communication between the left ventricle and the right atrium and is a serious complication of aortic infective endocarditis. Group B Streptococcus is an uncommon cause of in...
Transvaginal resection of a gastrointestinal stromal tumor of the rectum: a case report
The most common curative treatment for gastrointestinal stromal tumors (GISTs) is local excision. For rectal GISTs, however, local excision is difficult because of the anatomical features of the rectum. The op...
Clinical complete response after trastuzumab deruxtecan 6th-line treatment for postoperative gastric cancer recurrence: a case report
Despite the recent developments in the treatment of advanced or recurrent gastric cancer, the median survival time remains shorter than 15 months. Herein, we report a case of postoperative gastric cancer recur...
Late-onset lethal complication of non-surgically managed massive gastric conduit necrosis after esophagectomy: a case report
Gastric conduit necrosis (GCN) after esophagectomy is a serious complication that can prove fatal. Herein, we report a rare case of GCN with a severe course that improved with conservative treatment.
Gastric rupture caused by intragastric perforation of splenic artery aneurysm: a case report and literature review
The rupture of splenic artery pseudoaneurysm (SAP) is life-threatening disease, often caused by trauma and pancreatitis. SAPs often rupture into the abdominal cavity and rarely into the stomach.
A successful complete resection for multidrug-resistant giant gastrointestinal stromal tumor invading the transverse colon with multiple liver metastases in a young female: a case report
Gastrointestinal stromal tumors (GISTs) are rare in young people and are often detected after becoming symptomatic or at an advanced stage. Herein, we report a case of complete reduction surgery for a substant...
Minimally invasive elective gastrectomy after preoperative chemotherapy in a patient with frailty who presented with locally far advanced-stage gastric cancer: a case report
Herein, we report a case of gastric antrum cancer with multiple invasions to other organs that was completely cured with laparoscopic distal gastrectomy after preoperative chemotherapy in a patient with poor g...
Appendiceal neoplasms derived from appendiceal tip remnants following appendectomy: a report of two cases
Neoplasms derived from remnant appendix are rarely described, with most cases arising from the appendiceal “stump”. Here, we present two surgical cases of appendiceal neoplasms derived from appendiceal “tip” r...
Migrated tubal sterilisation clip presenting as a subcutaneous gluteal foreign body 24 years later: a case report and literature review
The incidence of sterilisation clip migration is reportedly 25%. However, less than 1% of those who experience clip migration will present with pain, an abscess, or spontaneous extrusion. Here we present a rar...
Repair of a right coronary artery rupture with perforated right ventricle following spontaneous pseudoaneurysm: a case report
Following the rupture of a coronary artery, a patient’s condition usually deteriorates rapidly due to cardiac tamponade. A pseudoaneurysm due to a coronary artery rupture is rare; however, when a spontaneous c...
Totally thoracoscopic atrial fibrillation surgery following massive small bowel resection due to superior mesenteric artery embolization: report of two cases
Thromboembolic occlusion of the superior mesenteric artery (SMA) is a grave complication in individuals diagnosed with atrial fibrillation (AF). This condition often necessitates extensive bowel resection, cul...
Laparoscopic left hepatectomy for a patient with an absence of portal bifurcation using real-time imaging: a case report
Absence of portal bifurcation is an extremely rare anomaly that should be recognized preoperatively, especially prior to a major hepatectomy.
A case of pseudo-Kaposi sarcoma with chronic limb-threatening ischemia
Pseudo-Kaposi sarcoma (PKS) is a rare vascular proliferative disease, caused by arteriovenous malformation (AVM) and chronic venous insufficiency. The lesions are characterized by purple or reddish-brownish pa...
Successful R0 resection after chemotherapy, including nivolumab, for gastric cancer with liver metastases: three case reports
Advances in chemotherapy have increased clinical experience with conversion surgery for inoperable advanced gastric cancer. This report describes three patients with unresectable gastric cancer accompanied by ...
A case of surgical treatment for recurrence of right ventricular metastasis due to renal cell carcinoma after molecular targeted therapy
Cardiac metastasis including the right ventricle from renal cell carcinoma is rare. No standard treatment for cardiac metastasis and recurrence in renal cell carcinoma has been established.
Spontaneous rupture of a mycotic splenic artery pseudoaneurysm secondary to histoplasmosis: a case report
A splenic artery pseudoaneurysm is a rare pathology that occurs mainly secondary to pancreatitis, abdominal trauma, peptic ulcers, pancreatic and gastric cancers, and infections. It is best diagnosed using com...
Laparoscopic repair of a primary parahiatal hernia combined with gastric volvulus: a case report and literature review
Parahiatal hernias present a hernial orifice at the diaphragm that is adjacent to the esophageal hiatus, differing from the paraesophageal type of hiatal hernias. Although diagnostic imaging has advanced in re...
The Correction to this article has been published in Surgical Case Reports 2024 10 :161
Sarcomatoid malignant pleural mesothelioma: a case of long-term recurrence-free survival following curative intent surgery alone
Curative intent surgery may be indicated for some patients with resectable early stage malignant pleural mesothelioma (MPM). However, sarcomatoid MPM is a highly aggressive subtype for which curative intent su...
A pediatric case of Burkitt’s lymphoma with bile duct obstruction requiring surgical biliary reconstruction
Biliary obstruction due to compression by a B-cell solid tumor occurs rarely. A few reports have described biliary reconstruction surgery for obstructive jaundice caused by Burkitt’s lymphoma. However, there a...
Laparoscopic surgery for De Garengeot’s hernia in a man after inguinal hernia surgery with a mesh plug: a case report and review of literature
De Garengeot’s hernia is a rare case of a femoral hernia that contains the appendix. Here we report a case of De Garengeot’s hernia that occurred in a male patient who had a history of inguinal hernia surgery ...
Thoracoscopic enucleation of an esophageal glomus tumor in the prone position: a case report and literature review
Glomus tumors (GT) generally occur in the skin. However, esophageal GT, an extremely rare condition, has no established standardized treatment guidelines. Herein, we report the case of an esophageal GT success...
Surgical treatment for pulmonary metastasis from ovarian cancer: a retrospective case series
Distant metastases of ovarian cancer are rarely detected alone. The effectiveness of surgical intervention for pulmonary metastases from ovarian cancer remains uncertain. This study aimed to investigate the cl...
Emergency right lower lobectomy for severe pulmonary abscess in a pregnant woman at the 25th week of gestation: a case report
Pulmonary abscess is a severe infection commonly seen in patients with chronic obstructive pulmonary disease, interstitial pneumonia, immune deficiency disease, drug-induced immunocompromised state, and congen...
Subtotal esophagectomy and concurrent reconstruction with free jejunal flap for primary esophageal cancer after pancreatoduodenectomy
Pancreatoduodenectomy and subtotal esophagectomy are widely considered the most invasive and difficult surgical procedures in gastrointestinal surgery. Subtotal esophagectomy after pancreatoduodenectomy is exp...
Case of functional paraganglioma with intraoperative hypertensive crisis during robot-assisted thoracoscopic resection
Mediastinal paragangliomas are rare. Their dangerousness may unfold during surgery, especially if hormonal activity was previously unknown. We report our experience with this case in context to the incidence a...
Tuberculous peritonitis after conservative treatment for acute perforated appendicitis: a case report
Interval appendectomy is widely recommended for patients with abscesses due to perforated appendicitis. A concomitant malignancy-related problem was reported after conservative treatment of acute appendicitis ...
A first report of right-hemicolectomy for ascending colon cancer in Japan with the da Vinci SP surgical robot system
The da Vinci SP robotic surgical system received regulatory approval for use in colorectal cancer surgery in Japan in April 2023. Given the advantages of the precision of a robot and the postoperative cosmesis...
A case of abdominal aortic aneurysm presenting as symptomatic disseminated intravascular coagulation treated with endovascular aneurysm repair and postoperative administration of Nafamostat mesylate
Cases of abdominal aortic aneurysm discovered as purpura on the extremities with disseminated intravascular coagulation (DIC) are rare. The number of currently established strategies for the control of DIC wit...
Stage IV gastric adenocarcinoma with enteroblastic differentiation with 5-year relapse-free survival after D2 gastrectomy and chemotherapy: A case report
Gastric adenocarcinoma with enteroblastic differentiation (GACED), a rare subtype of gastric cancer, is associated with a more aggressive behavior than conventional gastric adenocarcinomas. We report a rare ca...
Idiopathic superior mesenteric venous thrombosis requiring bowel resection: a report of four cases
Superior mesenteric venous thrombosis (SMVT) is mostly treated with anticoagulation therapy; however, SMVT can lead to irreversible bowel ischemia and require bowel resection in the acute or subacute phase.
Malignant perineurioma derived from the retroperitoneum with an aggressive clinical course: a case report
Malignant perineurioma is a rare malignant counterpart of perineurioma derived from perineural cells. Resection is the primary option for the treatment of malignant perineuriomas; however, patients often devel...
Laparoscopic transabdominal approach for resection of presacral epidermoid cyst in an obese man: a case report
Complete resection of presacral epidermoid cysts is recommended due to the potential for infection or malignancy. Transsacral and transabdominal approaches have been used to treat presacral tumors. However, th...
Hepatic hemangioma in a simple liver cyst mimicking biliary cystic neoplasm
Follow-up is recommended for an asymptomatic unilocular hepatic cystic lesion without wall-thickness and nodular components. A few liver cystic lesions represent biliary cystic neoplasms, which are difficult t...
Laparoscopic cholecystectomy for patients with accessory liver lobe attached to the wall of the gallbladder: case reports
Laparoscopic cholecystectomy (LC) is one of the most commonly undertaken procedures worldwide for cholecystolithiasis and cholecystitis. Accessory liver lobe (ALL) is a developmental anomaly defined as an exce...
Secondary ileal lymph node metastases from rectal cancer: a case report
Colorectal cancer can invade adjacent organs, but rarely metastasizes to the regional lymph nodes (LNs) of the invaded organ. Herein, we report a case of rectal cancer invading the ileum and metastasized to th...
Perineoplasty for anal incontinence after obstetric anal sphincter injury repair: a case report
The rectal and vaginal walls are typically sutured if severe perineal lacerations with rectal mucosal damage occur during vaginal delivery. In case of anal incontinence after the repair, re-suturing of the ana...
Editorial Board
Sign up for article alerts and news from this journal
Affiliated with
An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
Publications
Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
Advanced Search
Journal List
v.113(3); May-Jun 2016
Preoperative Evaluation of the Surgical Patient
Primary care physicians and specialists are frequently involved in the care of surgical patients. Changes in reimbursement have prompted re-examination of preoperative testing and health care expenditures. Physicians have additional incentives to improve health care delivery and reduce costs. The perioperative surgical home concept involves coordinating all aspects of patient care, including behavioral modifications, during the perioperative period. Evidence-based guidelines on preoperative evaluation are available to assist practitioners in managing cardiovascular disease, and communicating surgical risks. Shared decision making in the preoperative period can improve surgical outcomes and patient satisfaction.
Introduction
In the United States, $937 billion was spent on hospital care in 2013 (the most recent year for which data is available), two-thirds of which was related to surgical services. 1 Approximately 100 million surgeries are performed each year in the U.S., over half of which are done in ambulatory facilities. As the elderly population increases, surgical volume has also been increasing as more procedures are being performed on older patients with multiple chronic medical conditions. Forty-three percent of all surgical procedures are paid for by Medicare or Medicaid.
Since the Affordable Care Act (ACA) was signed into law in 2010, two of its primary aims have been to improve health care delivery and reduce costs. To this end, there has been a renewed focus on moving from the high costs and fragmented care associated with the traditional volume-based fee for service model to more efficient systems of multidisciplinary coordinated health care delivery. The Patient Centered Medical Home (PCMH) is a well-established concept that designates one physician to coordinate all aspects of the patient’s care and has been shown to improve outcomes and patient satisfaction. 2 A similar model of coordinated care for surgical patients is the Perioperative Surgical Home (PSH), a multidisciplinary system designed to shepherd patients through the surgical process from the time that surgery is planned until 30 days after discharge. 3 Recent changes in reimbursement have provided incentives for physicians and hospitals to streamline surgical care and meet performance benchmarks such as reducing the rate of readmission for Medicare beneficiaries. 4 These changes have provided rich opportunity for primary care physicians and specialists to improve surgical outcomes by participating in the management and optimization of their patients in the days and weeks leading up to surgery.
Preoperative Evaluation
Preoperative evaluation is a process of clinical assessment that precedes the delivery of anesthesia care for surgery and non-surgical procedures. At the very least, it includes a review of medical records and recent test results, a comprehensive medical history, and a physical examination of the cardiovascular system, the pulmonary system, and the airway. As the preoperative evaluation is considered a basic element of anesthetic care, it is often performed in the immediate preoperative period (ie, on the day of surgery), by the anesthesiologist. However, the American Society of Anesthesiologists Task Force on Preanesthesia Evaluation recommends that patients with high disease severity and those undergoing procedures with high surgical invasiveness be evaluated prior to the day of surgery. 5
Preoperative Testing
There is no clear consensus on the optimal content and timing of a preoperative evaluation, but it is important to balance the potential benefits of preoperative testing with the known risks and costs. Although preoperative studies and tests are often ordered on a selective basis to guide or optimize perioperative management, routine preoperative testing (ordering tests in the absence of a specific clinical indication or purpose) is generally not recommended, especially prior to low risk surgery. 5 Testing of asymptomatic patients can result in a waste of limited health care resources, unnecessary postponement or cancellation of surgery or, at worst, additional diagnostic testing and harmful medical interventions in the name of preoperative clearance for surgery. 6 Conversely, substantial cost savings can result from the avoidance of unnecessary preoperative medical testing and office visits prior to low risk procedures such as cataract surgery.
One of the most commonly performed elective procedures in the U.S., cataract surgery accounts for yearly health care expenditures totaling 3.5 billion dollars, 80% of which are paid for by Medicare. 7 A safe procedure of short duration, cataract surgery carries less that a 1% risk of a major adverse cardiac event (MACE) or death, even in older patients with multiple chronic medical conditions. Surgery for cataracts is thought to be no more stressful than dental work or even activities of daily living. The majority of these procedures are performed in an ambulatory setting and are done with topical anesthesia and only light sedation. Although it carries low risk, more than half of Medicare patients who underwent cataract surgery in 2012 had at least one preoperative test performed, despite evidence that routine testing before cataract surgery does not reduce adverse events or improve outcomes. 8 , 9 The extent of preoperative testing has been shown to depend more on individual opthalmologists’ practice patterns rather than adherence to published, evidence-based guidelines on preoperative testing. Therefore, selective preoperative testing should be guided by medical history and physical exam findings rather than a matter of routine practice.
ACC/AHA Guidelines
In 2014, the American Heart Association and American College of Cardiology updated their guidelines on cardiovascular evaluation and management of patients undergoing non-cardiac surgery. 10 The purpose of the guidelines is to
provide patients and their caregivers with evidence-based information about perioperative cardiovascular risk; and
guide management of patients with cardiovascular conditions and comorbidities.
Risk Assessment
Procedures such as cataracts, superficial plastic surgery, and endoscopy are considered low risk procedures because they carry less than a 1% chance of a major adverse cardiac event (MACE) including death or a myocardial infarction in the perioperative period. 10 Elevated risk applies to procedures that carry a risk of MACE equal to 1% or greater. The degree of risk depends on procedural and patient factors and can be estimated with the Revised Cardiac Risk Index (RCRI), a validated tool to predict the risk of major cardiac complications. 11 , 12 (See Table 1 ). A patient who has 0 or 1 of the 6 RCRI risk factors is considered to be at low risk for MACE. Two or more risk factors confers elevated risk of MACE. Other validated risk calculators have also been used to predict procedure-specific risks. 13 , 14 These tools can be used to determine whether further preoperative evaluation is appropriate.
Revised Cardiac Risk Index
Revised Cardiac Risk Index
Risk of major adverse cardiac event (MACE): 0 risk factors: 0.4%; 1 risk factor 0.9%; 2 risk factors 6.6%; 3 or more 11%
Management of Coexisting Disease
Coronary artery disease.
Coronary artery disease (CAD) increases the risk of perioperative morbidity and mortality, especially in the context of a recent myocardial infarction (MI) or coronary revascularization (CABG or PCI). For patients who have had a recent MI (within six months), the risk of both MACE and mortality is highest in the first 30 days following the MI (32.8% and 14.2%, respectively). 15 These patients are also at an eight-fold increased risk of stroke. 16 It is therefore recommended that elective, non-cardiac surgery be delayed for at least 60 days following an MI without coronary intervention.
Many patients with coronary artery disease who have had percutaneous coronary intervention (PCI) with balloon angioplasty or coronary artery stents present for non-cardiac surgery. 17 Up to 26% of patients with either a bare metal stent (BMS) or drug-eluting stent (DES) will require surgery within five years of undergoing PCI. 18 Drug eluting stents offer more protection than BMS against re-stenosis from smooth muscle proliferation but are slower to re-endothelialize and thus require a longer period of dual anti-platelet therapy (DAPT) to prevent life threatening stent thrombosis. It is known that premature discontinuation of DAPT increases the risk of stent thrombosis, especially in patients undergoing surgery, which induces a hypercoagulable state. The risk of MACE is highest (10.5%) in those patients with BMS who undergo surgery within 30 days after PCI, and lowest (2.8%) in those who wait at least 90 days. 19 Another study found that MACE was highest when major non-cardiac surgery was performed less than 45 days after implantation of any coronary stent. 20 Following placement of a DES, the risk of MACE is lowest in those who wait at least 365 days before non-cardiac surgery. In both cases, the risk of MACE is higher when surgery is performed on an emergent basis. For patients undergoing surgery prior to completion of DAPT, the theoretical risk of surgical bleeding while on DAPT must be balanced with the risk of stent thrombosis if dual antiplatelet therapy is held for surgery. Decisions about management of DAPT should be made in concert with the patient’s cardiologist. The updated ACC/AHA guidelines recommend delaying elective non-cardiac surgery for 14 days following balloon angioplasty, at least 30 days following BMS implantation, and 365 days following DES implantation, although in some cases a waiting period of 180 days after DES implantation may be appropriate.
Medical Decision-Making
For practitioners involved in the evaluation of patients with coronary artery disease preparing for surgery, a stepwise approach is available to assist in patient evaluation and estimation of risk. (See Figure 1 ). Patients who are planning surgery with low risk of MACE and those at elevated risk of MACE with at least moderate functional capacity (>4 METS as defined by the ability to climb a flight of stairs without stopping, walking uphill with ease, or gardening) can proceed to surgery without further evaluation. Patients with poor or unknown functional capacity may benefit from pharmacologic stress testing if it will influence their decision to have surgery or change perioperative management. Patients who elect to undergo stress testing may be candidates for coronary angiography or revascularization prior to surgery. Similar recommendations are available for managing patients with heart failure, arrhythmias, and heart valve disease. 10
Stepwise Approach to Perioperative Cardiac Assessment: Treatment Algorithm.
As part of any assessment of cardiovascular health, it is important to differentiate between active cardiac conditions and stable clinical risk factors. Patients with active cardiac conditions (acute coronary syndromes, decompensated heart failure, significant arrhythmias, or severe valvulopathy) are at high risk for perioperative MACE and should be evaluated and treated according to guideline-directed medical therapy. 21 For those with clinical risk factors (history of CVA, history of ischemic heart disease, history of congestive heart failure, diabetes, or kidney failure), the revised cardiac risk index or a similar risk calculator should be used along with procedural factors to estimate the risk perioperative MACE prior to surgery.
Additional tests and studies such as electrocardiograms (ECGs), chest x-rays, and blood tests are often ordered as a matter of routine—actions that are often based on medicolegal concerns or perceived expectations rather than on evidence based guidelines. 22 Twelve lead ECGs may be informative in patients with known cardiovascular disease, but are not indicated for asymptomatic patients undergoing low risk procedures. 10 As many as 45% of asymptomatic patients have abnormal ECG findings. 5 There is also no agreed upon minimum age requirement for ECG testing among asymptomatic patients. Similarly, chest x-rays were once included as part of any preoperative evaluation, but abnormal findings may be present in up to 60% of asymptomatic patients and can lead to costly and unnecessary postponement or cancellation of surgery, changes in medical management that otherwise would not have occurred, and excess radiation exposure. The same is true of laboratory tests such as hemoglobin and hematocrit measures, serum chemistries, and coagulation profiles. It is now recommended that these tests should only be ordered when clearly indicated (i.e., to answer a specific question and only if it will lead to a change in management).
Medications
Many patients with cardiovascular disease presenting for preoperative evaluation are on chronic antihypertensive therapy. The use of beta adrenergic antagonists (beta blockers) has been the subject of several studies in recent years. 23 , 24 It is now recommended that patients who are on chronic beta blocker therapy remain so throughout the perioperative period. For beta blocker naive patients, beta blockers may reduce perioperative cardiac risk, but are associated with adverse effects such as bradycardia, hypotension, and stroke. Therefore, initiating beta blocker therapy on the day of surgery is not recommended. Patients taking angiotensin-converting enzyme (ACE) inhibitors or angiotensin-receptor blockers (ARBs) on the day of surgery may experience transient hypotension, but are at no increased risk of adverse cardiac events, and continuing these medications in the perioperative period is reasonable. 10
Early Patient Engagement and Prehabilitation
One strategy to reduce length of stay and prevent postoperative complications is the concept of early patient engagement in the preoperative period or “prehabilitation” (enhancing functional capacity in preparation for a stressful event such as surgery). 25 This is especially relevant to elderly patients with chronic respiratory disease who are at increased risk for postoperative pulmonary complications, which they tolerate poorly. Ergina et al. reported that identifying patients with COPD who smoke and have poor functionality and instituting perioperative regimens that include smoking cessation, bronchodilators, chest physiotherapy, postural drainage, and deep breathing exercises reduced the incidence of postoperative pulmonary complications. 26 Other investigators have reported on the benefits of preoperative aerobic exercise training on postoperative recovery from colorectal surgery. 27 , 28 Others have shown that prehabilitation programs have a positive impact on length of stay and health-related quality of life measures. 29
Smoking Cessation
Despite the long-known health risks of tobacco use, 19.2% of American adults report smoking every day or some days. 30 Tobacco-related diseases are the leading cause of preventable deaths worldwide, contributing to 443,000 deaths per year in the U.S. and nearly $200 billion annually in medical expenses and lost productivity. 31 One half of people who continue to smoke will die of a tobacco-related illness. Lung cancer is the most prevalent type of cancer in the world and the leading cause of cancer death in the United States, accounting for 27% of the expected 589,000 U.S. cancer deaths in 2015. The majority of lung cancer deaths are caused by smoking.
The benefits of smoking cessation prior to surgery are well known. Within hours of stopping, blood levels of carbon monoxide and nicotine decline, leading to improved blood flow and oxygen delivery to tissues. 32 , 33 After several weeks, some aspects of airway inflammation and hyperreactivity improve, including mucociliary clearance, symptoms of coughing and wheezing, and the decline of pulmonary function as measured by lung spirometry. Conversely, patients who continue to smoke in the perioperative period are at increased risk for infection and impaired wound healing, as well as perioperative pulmonary complications such as respiratory failure requiring unplanned ICU admission, pneumonia, and airway complications related to anesthesia. The precise amount of time required to fully realize the benefits of smoking cessation are unknown, with some requiring up to 6 months, and even brief periods of cessation are helpful, but longer is assumed to be better. 33 A recent review of the literature found that compared with current smokers, those who abstain from smoking for at least four weeks (and preferably for at least eight weeks) prior to surgery experience lower rates of respiratory complications and fewer instances of impaired wound healing. 34
Surgery presents a unique opportunity for health professionals to encourage smoking cessation. A teachable moment occurs when a patient is faced with the recent diagnosis of a serious illness or the prospect of surgery. 35 Quit rates are higher following major surgery, especially surgery related to conditions associated with smoking. Heightened awareness of risks and potential negative consequences may provide additional motivation to reduce or quit smoking and patients may be more receptive to anti-smoking discussions, especially when initiated by a physician or other health care professional. 32
For surgical patients (and non-surgical patients) who are willing to make a quit attempt and be smoke-free for surgery, and for the physicians who care for them, there are effective smoking cessation resources available in the form of tobacco dependence counseling and medication treatments. 36
The Brief Intervention is a practical tool that busy clinicians can use during a routine preoperative clinic visit. 37 It is effective in reducing smoking rates in surgical patients and is based on the “5 A” model for reducing tobacco use and dependence: Ask—“Do you smoke?” and “Do you want to quit?” Advise— Strongly urge all tobacco users to quit. Assess—Determine willingness to make a quit attempt. Assist—Provide counseling and medication. Arrange—Ensure follow-up contact. Although intensive behavioral counselling that involves problem solving training and social support is most effective, national telephone tobacco quitlines (1-800-QUIT-NOW) and web-based resources ( http://www.smokefree.gov ) are also useful. 38 Smoking cessation counseling is effective even for those not yet willing to make a quit attempt. 39
All patients attempting to quit smoking should be encouraged to use effective first line medications unless medically contraindicated (e.g., Bupropion SR, varenicline, and nicotine replacement therapy, which includes gum, lozenges, and patches). When used together, tobacco dependence counseling and medications are most effective in increasing quitting success and reducing withdrawal symptoms. 40
Evidence-based smoking cessation strategies are not only efficacious, but are also cost effective and consistent with the Healthy People 2020 objective of reducing the prevalence of cigarette smoking among U.S. adults to less than 12%. To this end, the 2010 Patient Protection and Affordable Care Act provides expanded coverage for evidence-based smoking cessation treatments.
The preoperative evaluation offers physicians and other health care professional a unique opportunity to help patients optimize their health prior to surgery. Updated, evidence-based guidelines can assist providers in selecting the most appropriate methods of patient evaluation while making the most efficient use of limited health care resources. This includes encouraging healthy behavioral modifications. It is important to bear in mind that the patient always has the final say in any decision to undergo surgery. Therefore, these guidelines are best used to aid shared decision-making, taking into consideration the patient’s perspective on the risks and benefits of surgery.
Frederick T. O’Donnell, MD, is in the University of Missouri-Columbia Health Care Department of Anesthesiology and Perioperative Medicine.
Contact: ude.iruossim.htlaeh@fllennodo
None reported.
- Google Chrome
Intended for healthcare professionals
My email alerts
BMA member login
Username * Password * Forgot your log in details? Need to activate BMA Member Log In Log in via OpenAthens Log in via your institution
Search form
Advanced search
Search responses
Search blogs
How to present patient...
How to present patient cases
Related content
Peer review
Mary Ni Lochlainn , foundation year 2 doctor 1 ,
Ibrahim Balogun , healthcare of older people/stroke medicine consultant 1
1 East Kent Foundation Trust, UK
A guide on how to structure a case presentation
This article contains...
-History of presenting problem
-Medical and surgical history
-Drugs, including allergies to drugs
-Family history
-Social history
-Review of systems
-Findings on examination, including vital signs and observations
-Differential diagnosis/impression
-Investigations
-Management
Presenting patient cases is a key part of everyday clinical practice. A well delivered presentation has the potential to facilitate patient care and improve efficiency on ward rounds, as well as a means of teaching and assessing clinical competence. 1
The purpose of a case presentation is to communicate your diagnostic reasoning to the listener, so that he or she has a clear picture of the patient’s condition and further management can be planned accordingly. 2 To give a high quality presentation you need to take a thorough history. Consultants make decisions about patient care based on information presented to them by junior members of the team, so the importance of accurately presenting your patient cannot be overemphasised.
As a medical student, you are likely to be asked to present in numerous settings. A formal case presentation may take place at a teaching session or even at a conference or scientific meeting. These presentations are usually thorough and have an accompanying PowerPoint presentation or poster. More often, case presentations take place on the wards or over the phone and tend to be brief, using only memory or short, handwritten notes as an aid.
Everyone has their own presenting style, and the context of the presentation will determine how much detail you need to put in. You should anticipate what information your senior colleagues will need to know about the patient’s history and the care he or she has received since admission, to enable them to make further management decisions. In this article, I use a fictitious case to …
Log in using your username and password
BMA Member Log In
If you have a subscription to The BMJ, log in:
Need to activate
Log in via institution
Log in via OpenAthens
Log in through your institution
Subscribe from £184 *.
Subscribe and get access to all BMJ articles, and much more.
* For online subscription
Access this article for 1 day for: £33 / $40 / €36 ( excludes VAT )
You can download a PDF version for your personal record.
Buy this article
Recent Search Keywords
Surgical Case Reports
Review Time
Publish time, about journal scr.
Surgical Case Reports (SCR) the renowned official journal. Dive into a comprehensive collection of gastroenterological surgery, cardiovascular surgery, thoracic surgery, and more. Our open-access platform, supported by rigorous peer-review processes, showcases novel treatments and unique surgical experiences from around the globe.
The journal aims to develop and uphold the highest research standards, to provide a scope for evidence-based treatments through the publication of quick review papers and special issues, and to contextualise the findings through the publication of editorials, commentaries, and letters from the surgical community. We enforce reporting guidelines and require that all research involving human participants be registered in a public access research database.
From transplant surgery insights to rare breast and endocrine surgery tales, SCR is committed to advancing the realm of surgical science. By encapsulating unique cases and innovative treatments, we aim to foster a rich educational forum for clinicians and researchers alike.
Scope of Journal
Surgical Case Reports (SCR) is a dedicated platform aiming to advance the understanding and practice of surgery. Our principal goal is to provide a global forum where clinicians, surgeons, and researchers can share, learn, and discuss novel surgical techniques, treatments, and patient case studies that contribute to the field's progress.
Submit Manuscript
For submission authors can directly submit manuscript to [email protected] . If you want to proceed with online submission you can follow the below link. You will need to be a register user to submit your manuscript.
Submit Online
General Information
Manuscripts number will be provided to the corresponding author within 72 hours for the respective manuscript submitted.
• 14 days review process with international peer-review standards
• Timeline of processing from Submission to Publication is 30 days
• Manuscript will be published within 7 days of acceptance
Open Access
All the work at Surgical Case Reports is licensed under a Creative Commons Attribution 4.0 International License. Authors at Surgical Case Reports retain copyright to their work and allow others to copy, distribute, transmit, and adapt their work, provided proper attribution is given.
We follow Creative Commons 'Attribution' licence (CC BY) . This license lets others distribute, remix, tweak, and build upon your work, even commercially, as long as they credit you for the original creation. View License Deed | View Legal Code
Indexing and Abstract
All articles are made open access to maximise the long-term visibility, impact and influence of our content.
• AcademicPub
• The British Library
• Cancerlit
• Google Scholar
• Medline/PubMed
• Science Citation Index Expanded
• Scisearch
• Web of Science
• Emerging Sources Science Citation Index
About Journal
Peer review process, editorial board, article processing charge, article in press, current issue.
Peer Review
Highest quality of international peer review standard
Initial submission.
Select the right journal and submit your manuscript.
Manuscript Number
Our editors will communicate and send you the manuscript number. We officially begin processing your manuscript.
First Decision
Based on the outcome of the peer-review you would receive review comments from the international experts on your subject.
APC Invoicing
We will share the invoice that can be paid online using credit card or bank transfer. We also have option to convert the invoice in the desired currency.
Proofing & Correction
Once you are aware of the review comments then you can make minor changes based on the inputs and any corrections that should be done before we move ahead.
Indexing & Archiving
If your research is not easy to find, it cannot help advance science or scientific society. Post-publication of your research, indexing is the most important things we do at Surgical Case Reports. We aim to make all articles published with Surgical Case Reports easy to find by the widest audience and also work with search engines, social media platforms and scholarly communication networks.
Masks Strongly Recommended but Not Required in Maryland, Starting Immediately
Due to the downward trend in respiratory viruses in Maryland, masking is no longer required but remains strongly recommended in Johns Hopkins Medicine clinical locations in Maryland. Read more .
Vaccines
Masking Guidelines
Visitor Guidelines
Center for Bloodless Medicine and Surgery
Case study: surgical oncology, renal retroperitoneal mass adherent to the inferior vena cava with blood conservation by cell saver and intraoperative normovolemic hemodilution (ianh).
A 68-year old woman who is one of Jehovah’s Witnesses presented with general malaise and some left upper quadrant pain and nausea. Her history was significant for a right nephrectomy for renal cell carcinoma 15 years ago. A CT scan revealed a heterogeneous mass located in the right-sided retroperitoneal space measuring 8 by 11 cm with compression of the inferior vena cava (IVC) and effacement of the gallbladder. In addition, she had a pacemaker implant 3 years prior, for the treatment of sick sinus syndrome.
Two surgeons, Dr. James Black from vascular surgery, and Dr. Mohamed Allaf from Urology as well as Dr. Steven Frank, the Medical Director of the Center for Bloodless Medicine and Surgery were consulted. Drs. Frank and Allaf saw her at the same time together, along with her family members, to map out an intraoperative plan. On reviewing the CT scans, the three physicians decided that a surgical resection would be high-risk, given the involvement of the vena cava, and that the risk of bleeding was significant. The risks and benefits of the procedure, as well as the available blood conservation techniques were discussed with the patient and her family. It was decided that by using autologous blood salvage (Cell Saver), along with a special leukoreduction filter, the risks would be minimized and the planned procedure could be accomplished. Intraoperative autologous normovolemic hemodilution (IANH) was also discussed as a blood conservation technique and the patient agreed this was acceptable to minimize risks.
The preoperative hemoglobin level was 14.7 g/dL, which was thought to be adequate for this surgical procedure. The anesthesia plan was developed by Dr. Frank, which included a thoracic epidural to minimize both postoperative pain and the requirement for narcotic pain medications. Large bore venous access was placed after induction of general anesthesia, using three 8.5 French introducers, 2 in the right and 1 in the left internal jugular veins. An intra-arterial catheter was also placed in the radial artery for continuous blood pressure monitoring. This degree of venous access would allow for veno-veno bypass from the iliac vein to the right atrium, if a vena cava cross clamp was necessary to remove the tumor. Prior to incision, 2 units of fresh whole blood were removed into CPDA anticoagulant bags, but remained in continuity with the patient’s circulation (via IV tubing) at all times. A volume expander (albumin) along with 2 liters of crystalloid solution were given for the hemodilution technique. Phenylephrine was given to maintain blood pressure during the IANH phlebotomy to allow the safe removal of autologous blood.
The surgery was performed through a right-sided thoraco-abdominal incision, and the diaphragm was taken down to provide access to the tumor. The tumor was identified and was adherent to the vena cava, but appeared to be resectable. A sidebiting cross clamp was applied to the cava, the tumor was removed, and the cava was repaired. There was no need for veno-veno bypass as the patient tolerated the partial cross clamp with hemodynamic stability. The blood loss was substantial (1,200 mLs) which for her body mass (50kg) was about 1/3 of her entire blood volume (calculated as 70 mL per kg or 3,500 mLs). The shed blood was processed through the Cell Saver and returned to the patient using the leukoreduction filter to minimize and chances of spreading tumor cells. The 2 units of autologous whole blood were given back to her near the end of the procedure. The closure included repair of the diaphragm and no chest tube was required.
On postoperative day #1 she was sitting up in a chair and on postoperative day #2 she was walking. A duplex ultrasound exam of the vena cava and iliac veins revealed good blood flow, and no narrowing or thrombosis. Pain scores and narcotic requirements were minimal due to the thoracic epidural. The pathology report came back as recurrent papillary renal cell carcinoma, with clean margins, indicating the tumor was completely resected. She was discharged to home on postoperative day #7 to be followed up by Oncology.
Open access
Published: 27 June 2024
Adverse postoperative outcomes in elderly patients with sarcopenia
No study has compared 30-day and 90-day adverse postoperative outcomes between old-age patients with and those without sarcopenia.
Patients and methods
We categorize elderly patients receiving major surgery into two groups according to the presence or absence of preoperative sarcopenia that were matched at a 1:4 ratio through propensity score matching (PSM). We analyzed 30-day or 90-day adverse postoperative outcomes and mortality in patients with and without sarcopenia receiving major surgery.
Multivariate logistic regression analyses revealed that the patients with preoperative sarcopenia were at significantly higher risk of 30-day postoperative mortality (adjusted odds ratio [aOR]. = 1.25; 95% confidence interval [CI]. = 1.03–1.52) and 30-day major complications such as postoperative pneumonia (aOR = 1.15; 95% CI = 1.00-1.40), postoperative bleeding (aOR = 2.18; 95% CI = 1.04–4.57), septicemia (aOR = 1.31; 95% CI = 1.03–1.66), and overall complications (aOR = 1.13; 95% CI = 1.00-1.46). In addition, surgical patients with sarcopenia were at significantly higher risk of 90-day postoperative mortality (aOR = 1.50; 95% CI = 1.29–1.74) and 90-day major complications such as pneumonia (aOR = 1.27; 95% CI = 1.10–1.47), postoperative bleeding (aOR = 1.90; 95% CI = 1.04–3.48), septicemia (aOR = 1.52; 95% CI = 1.28–1.82), and overall complications (aOR = 1.24; 95% CI = 1.08–1.42).
Conclusions
Sarcopenia is an independent risk factor for 30-day and 90-day adverse postoperative outcomes such as pneumonia, postoperative bleeding, and septicemia and increases 30-day and 90-day postoperative mortality among patients receiving major surgery.
Condensed abstract
No study has compared 30-day and 90-day adverse postoperative outcomes between patients with and those without sarcopenia. We conducted a propensity score?matched (PSM) population-based cohort study to investigate the adverse postoperative outcomes and mortality in patients undergoing major elective surgery with preoperative sarcopenia versus those without preoperative sarcopenia. We demonstrated that sarcopenia is an independent risk factor for 30-day and 90-day adverse postoperative outcomes, such as postoperative pneumonia, bleeding, septicemia, and mortality after major surgery. Therefore, surgeons and anesthesiologists should attempt to correct preoperative sarcopenia, swallowing function, and respiratory muscle training before elective surgery to reduce postoperative complications that contribute to the decrease in surgical mortality.
Peer Review reports
Introduction
Sarcopenia is defined as the progressive and generalized loss of skeletal muscle mass and strength with a risk of adverse outcomes, such as physical disability, poor quality of life, and even death [ 1 ]. Lifestyle, physical inactivity, malnutrition, and chronic diseases (e.g., osteoporosis and metabolic diseases) are all risk factors for sarcopenia [ 2 , 3 , 4 ]. Currently, the pathogenesis of sarcopenia is unclear. However, sarcopenia may be related to genetics, nutritional deficiencies, neuromuscular function, hormones, autophagy, mitochondrial abnormalities, and gut flora [ 5 , 6 ]. Sarcopenia not only increases the fall rate, disability rate, hospitalization rate, surgical complication rate, and even mortality but also affects the occurrence, development, and prognosis of various diseases [ 7 ]. However, research on sarcopenia is currently in the exploratory stage, and the association of preoperative sarcopenia with surgery is unclear.
The mass and strength of skeletal muscles are affected by various factors, such as age, gender, underlying diseases, dietary habits, and exercise, and can reflect the overall functional status [ 8 ]. In general, the prognosis of surgical patients is closely related to the functional status [ 9 ]. Patients with sarcopenia, as a special group, often exhibit low physical function, and they may be at an increased risk of postsurgical complications [ 10 , 11 ]. Moreover, sarcopenia can lead to a decrease in skeletal muscle and the weakening of respiratory and swallowing muscles, thereby resulting in atelectasis, pneumonia, dysphagia, and malnutrition [ 12 ]. These aforementioned factors may increase postoperative complications and mortality, prolong hospital stay, affect quality of life, and increase health-care costs [ 13 ]. Therefore, surgeons and anesthesiologists should pay increased attention to patients with sarcopenia, as a potential high-risk group for adverse postoperative outcomes.
The influence of preoperative sarcopenia on the prognosis of major postoperative outcomes is unclear. The findings of previous studies on the association of sarcopenia with adverse postoperative outcomes and mortality are conflicting, and studies with an adequate sample size, clear definition of sarcopenia, and satisfactory results are scant [ 13 , 14 , 15 , 16 ]. Therefore, large-scale clinical research should be conducted on the prognosis of postoperative outcomes in patients with sarcopenia by utilizing a real-world database. Therefore, we conducted a comparative study through PSM to estimate the effects of preoperative sarcopenia on the outcomes of elective surgery.
Data sources
We used data from January 2016 to December 2019 from Taiwan’s National Health Insurance (NHI) Research Database (NHIRD). The follow-up duration was from the index date to December 31, 2020. The NHIRD contains registration files and the original claims data of all NHI beneficiaries (i.e., approximately 27.38 million individuals). All NHIRD data, which are encrypted to ensure beneficiaries’ privacy, include detailed outpatient and inpatient claims information such as patient identification number; birth date; sex; diagnostic codes according to International Classification of Diseases, Ninth Revision, Clinical Modification ( ICD-9-CM ) and International Classification of Diseases, Tenth Revision, Clinical Modification ( ICD-10-CM ); treatment information; medical costs; dates of hospital admission and discharge; and date of death [ 17 , 18 , 19 , 20 , 21 ]. All data sets were interlinked using patient identification numbers. Our protocols were reviewed protocols were reviewed and approved by the Institutional Review Board of Tzu-Chi Medical Foundation (IRB109-015-B).
I would like to clarify that informed consent was waived in our study. This decision was made in accordance with the Personal Information Protection Act, as the data sets used in our research fall under its provisions.
Participant selection
We selected 254,222 elderly patients aged ≥ 60 years who underwent major elective inpatient surgery; these old-age patients required general, epidural, or spinal anesthesia and hospitalization for more than 1 day between 2016 and 2019 in Taiwan. The evaluation of CT scans was limited to the 12-month preoperative period. Among the selected patients, 12,158 patients with a diagnosis of sarcopenia and 242,067 without a diagnosis of sarcopenia were categorized into the sarcopenia and nonsarcopenia groups, respectively (Supplemental Table 1 ). Before 2016, because of a lack of consensus regarding the definition of sarcopenia, a variety of diagnostic criteria were used [ 22 ]. In October 2016, the US Centers for Disease Control and Prevention formally recognized sarcopenia as a disease and coded it as M62.84 in ICD-10-CM [ 23 ]. We defined sarcopenia according the ICD-10-CM code after 2016 [ 17 ]. At least two claims for patients with a principal diagnosis of sarcopenia within the 12-month preoperative period were defined as the criteria for sarcopenia diagnosis. In Taiwan, sarcopenia was coded according to the results of a previous Taiwan study [ 24 ]; sarcopenia was defined as the skeletal muscle mass index (SMI) of 2 standard deviations or more below the normal sex-specific mean values for young persons. The date of onset of diabetes was regarded as the index date. The SMI was calculated using the following formula: SMI = L3 skeletal muscle cross-sectional area (cm 2 )/height 2 (m 2 ), which was measured from computed tomography images [ 25 ].
PSM and covariates
After adjustment for confounders, we used a multivariate logistic regression model to assess 30-day or 90-day postoperative complications onset from the index date (surgical date) in patients with and without preoperative sarcopenia. To reduce the effects of potential confounders when comparing adverse postoperative outcomes between the sarcopenia and nonsarcopenia groups, we matched all patients through PSM according to the following variables: age, sex, income levels, urbanization, coexisting medical conditions, hospital level, type of anesthesia, ASA score, and surgical type (Table 1 ). We matched the cohorts at a ratio of 1:4 using a greedy matching method, and the covariates were matched within a caliper with a propensity score of 0.2 [ 26 ]. Comorbidities were determined according to ICD-9-CM codes in the main diagnosis records of inpatients or were defined if the number of outpatient visits was ≥ 2 within 1 year. Comorbidities that occurred 2 years before the index date were included in this study.
Continuous variables are presented as means ± standard deviations where appropriate. A PSM ratio of 1:4 was used for the preoperative sarcopenia and nonsarcopenia groups; this ratio is commonly used to select controls with identical background covariates to minimize the differences among participants (we considered using controls based on previous studies) [ 27 , 28 , 29 , 30 , 31 , 32 ]. A multivariate logistic regression model was used to analyze postoperative complications in surgical patients with and without preoperative sarcopenia [ 33 ]. Using multivariate logistic regression analysis, we calculated odd ratios (ORs) with 95% confidence intervals (CIs) to determine whether preoperative sarcopenia is a potential independent predictor of 30-day or 90-day postoperative complications.
Outcome measures
Eight major postoperative complications were monitored [ 28 ].: acute myocardial infarction, acute renal failure, deep-wound infection pneumonia, postoperative bleeding, pulmonary embolism, septicemia, and stroke. In our study, we utilized the Clavien Dindo classification system to categorize and describe postoperative complications, focusing on Grade 2 or higher complications [ 34 ]. The primary outcomes of this study were the complications and subsequent overall in-hospital mortality within 30 days after index surgery [ 27 , 28 , 29 , 30 , 31 , 32 ]. Studies have suggested that events recorded within 90 days of surgery are also postoperative complications [ 35 , 36 , 37 , 38 , 39 ].
Data analysis
We used χ 2 tests to analyze the descriptive parameters of demographic characteristics and coexisting medical conditions in the comparison of postoperative complications and death rates of patients with and without preoperative sarcopenia. Continuous variables were analyzed using t tests to compare the differences between patients with sarcopenia and controls. Multivariate logistic regression was used to analyze 30-day and 90-day postoperative complications and mortality between surgical patients with or without sarcopenia through the calculation of the adjusted ORs (aORs) with 95% CIs, with adjustment for age, sex, income level, urbanization, coexisting medical conditions, hospital level, type of anesthesia, ASA score, and surgical type. The logistic regression model’s goodness-of-fit was comprehensively assessed using both the Hosmer-Lemeshow test and the Omnibus test. The Hosmer-Lemeshow test evaluated the agreement between observed and expected outcomes across subgroups, while the Omnibus test assessed the overall significance of the model. These model fit assessments, including the results of the Hosmer-Lemeshow test and Omnibus test, ensured the validity and appropriateness of our logistic regression model. The statistical analysis software program V.9.4 (SAS Institute, Cary, North Carolina, USA) was used for data analyses; the differences between the groups were considered significant if two-sided P values were < 0.05.
Study cohort
The data of 60,790 surgical patients (i.e., 12,158 and 48,632 in the sarcopenia and nonsarcopenia groups, respectively) were included in this study for further analysis; their characteristics are listed in Table 1 . After frequency matching, the between-group differences in age, sex, income levels, urbanization, coexisting medical conditions, hospital levels, types of anesthesia, ASA scores, and surgical types were nonsignificant. The confounders (before matching) in the sarcopenia group significantly differed from those in the nonsarcopenia group ( p < .001; Supplemental Table 1 ). Compared with the nonsarcopenia group, the sarcopenia group had more individuals who were older, were female, had a low income, were rural residents, had more coexisting medical conditions, received surgery at medical centers, and received general anesthesia (Supplemental Table 1 ).
30-day or 90-day adverse postoperative outcomes
Patients with sarcopenia exhibited higher rates of 30-day postoperative complications, including postoperative pneumonia (1.18% vs. 0.93%; P = .0134), postoperative bleeding (0.09% vs. 0.04%; P = .0420), septicemia (0.76% vs. 0.53%; P = .0028), and overall complications (6.85% vs. 5.62%; P = .0162; Table 2 ). The 30-day postoperative mortality rates for surgical patients with and without sarcopenia were 1.21% and 0.94%, respectively ( P = .0085). Moreover, patients with sarcopenia exhibited higher rates of 90-day postoperative complications, including postoperative pneumonia (2.23% vs. 1.63%; P < .0001), postoperative bleeding (0.13% vs. 0.07%; P = .0267), septicemia (1.50% vs. 0.92%; P < .0001), and overall complications (8.85% vs. 7.95%; P = .0111). The 90-day postoperative mortality rates for surgical patients with and without sarcopenia were 2.08% and 1.38%, respectively ( P < .0001).
Adjusted ORs and 95% CIs for 30-day or 90-day adverse postoperative outcomes
After adjustment for age, sex, income levels, urbanization, coexisting medical conditions, hospital levels, types of anesthesia, ASA scores, and surgical types, our multivariate logistic regression analyses revealed that surgical patients with preoperative sarcopenia were at significantly higher risk of 30-day postoperative mortality (aOR = 1.25; 95% CI 1.03 to 1.52) and 30-day major complications, including postoperative pneumonia (aOR = 1.15; 95% CI = 1.00-1.40), postoperative bleeding (aOR = 2.18; 95% CI = 1.04–4.57), septicemia (aOR = 1.31; 95% CI = 1.03–1.66), and overall complications (aOR = 1.13; 95% CI = 1.00-1.46). In addition, surgical patients with sarcopenia were at significantly higher risk of 90-day postoperative mortality (aOR = 1.50; 95% CI = 1.29–1.74) and 90-day major complications, including postoperative pneumonia (aOR = 1.27; 95% CI = 1.10–1.47), postoperative bleeding (aOR = 1.90; 95% CI = 1.04–3.48), septicemia (aOR = 1.52; 95% CI = 1.28–1.82), and overall complications (aOR = 1.24; 95% CI = 1.08–1.42; Table 3 ).
Kaplan–Meier 30-day or 90-day postoperative mortality and complications
Figure 1 illustrates the cumulative risks of 30-day or 90-day postoperative mortality and complications in matched patients with and without sarcopenia. The cumulative 30-day postoperative mortality was significantly higher in the sarcopenia group than in the nonsarcopenia group ( P < .0001; Fig. 1 A), and the cumulative overall 30-day postoperative complications were significantly higher in the sarcopenia group than in the nonsarcopenia group ( P < .0001; Fig. 1 B). Moreover, the Kaplan–Meier curves revealed that the cumulative 90-day postoperative mortality and overall complications were significantly lower in the sarcopenia group than in the nonsarcopenia group ( P < .0001; Fig. 2 ).
Kaplan–Meier Estimates of 30-d Postoperative Mortality and 30-d Postoperative Complications Among Surgical Patients With and Without Sarcopenia. ( A ) 30-d Postoperative Mortality; ( B ) 30-d Overall Postoperative Complications
Kaplan–Meier Estimates of 90-d Postoperative Mortality and 90-d Postoperative Complications Among Surgical Patients With and Without Sarcopenia. ( A ) 90-d Postoperative Mortality; ( B ) 90-d Overall Postoperative Complications
Clinically, many patients with sarcopenia experience various challenges and severe complications of surgery [ 40 ]. However, the association of preoperative sarcopenia with adverse postoperative outcomes and mortality is unclear [ 13 , 14 , 15 , 16 ]. To the best of our knowledge, the present study is the first and the largest PSM-based comparative study on 30-day and 90-day adverse postoperative outcomes and mortality among patients with and without preoperative sarcopenia. This retrospective, real-world data-derived, population-based PSM cohort study revealed that preoperative existing sarcopenia is an independent risk factor for 30-day and 90-day adverse postoperative outcomes, such as postoperative pneumonia, postoperative bleeding, and septicemia, and preoperative sarcopenia is associated with increased 30-day and 90-day postoperative mortality among patients receiving major surgery. Multivariate logistic regression analyses revealed that surgical patients with preoperative sarcopenia were at significantly higher risk of 30-day postoperative mortality (aOR = 1.25; 95% CI = 1.03–1.52) and 30-day major complications, including postoperative pneumonia (aOR = 1.15; 95% CI = 1.00-1.40), postoperative bleeding (aOR = 2.18; 95% CI = 1.04–4.57), septicemia (aOR = 1.31; 95% CI = 1.03–1.66), and overall complications (aOR = 1.13; 95% CI = 1.00-1.46). In addition, surgical patients with sarcopenia were at significantly higher risk of 90-day postoperative mortality (aOR = 1.50; 95% CI = 1.29–1.74) and 90-day major complications, including postoperative pneumonia (aOR = 1.27; 95% CI = 1.10–1.47), postoperative bleeding (aOR = 1.90; 95% CI = 1.04–3.48), septicemia (aOR = 1.52; 95% CI = 1.28–1.82), and overall complications (aOR = 1.24; 95% CI = 1.08–1.42). Our results provide valuable comprehensive information on postoperative complications, especially postoperative pneumonia, postoperative bleeding, and postoperative septicemia, among patients with sarcopenia receiving surgery. Establishing a comprehensive protocol to prevent the aforementioned postoperative complications that contribute to surgical mortality can be valuable to future research.
Several reports have indicated similar outcomes [ 41 , 42 , 43 , 44 ], suggesting an association between preoperative sarcopenia and increased postoperative complications [ 41 , 42 , 43 , 44 ]. In our extensive investigation, we explored the impact of preoperative sarcopenia on postoperative outcomes within a cohort of 254,222 elderly patients (≥ 60 years) undergoing major elective inpatient surgery in Taiwan between 2016 and 2019. Utilizing Taiwan’s NHIRD, which includes detailed claims data for approximately 27.38 million individuals, our study stands out for its large cohort size, facilitating robust statistical analyses. Unlike earlier studies that employed diverse diagnostic criteria for sarcopenia, our research defined sarcopenia post-2016 using the ICD-10-CM code M62.84 and incorporated specific criteria based on the SMI derived from CT scans. This nuanced approach allows for a more precise identification of sarcopenic patients. Furthermore, our study employed PSM and multivariate logistic regression to account for potential confounders, ensuring a meticulous analysis of 30-day and 90-day postoperative complications. The investigation of eight major complications, including acute myocardial infarction, acute renal failure, deep-wound infection pneumonia, postoperative bleeding, pulmonary embolism, septicemia, and stroke, adds granularity to the understanding of the outcomes. Furthermore, the concentration on individuals aged 60 and above, along with the meticulous matching of different surgical procedures through PSM, distinguishes our approach. Unlike previous studies primarily focusing on specific surgical types, such as cardiac or abdominal surgery [ 43 , 44 ], our research expands the scope and enhances external validity due to a larger and more diverse sample [ 41 , 42 , 43 , 44 ]. Consequently, our conclusions elucidate a higher incidence of surgical complications among elderly individuals with sarcopenia, providing unique insights beyond the existing literature. Importantly, we extend our analysis beyond the conventional 30-day acute complications to include 90-day subacute complications, a novel contribution to the field. This study significantly advances our understanding of the intricate relationship between sarcopenia and postoperative outcomes, making a substantial and novel addition to the existing literature [ 41 , 42 , 43 , 44 ]. Our investigation not only scrutinizes acute complications within the conventional 30-day timeframe but extends its analysis to encompass subacute complications occurring within 90 days—a novel aspect absent in prior literature [ 41 , 42 , 43 , 44 ]. This extended timeframe provides a more comprehensive understanding of the postoperative complications associated with sarcopenia in the elderly, offering unique insights and a substantial addition to the existing literature.
The primary endpoints of our study were centered on complications and overall in-hospital mortality within 30 days following the index surgery, as supported by relevant literature [ 27 , 28 , 29 , 30 , 31 , 32 ]. Recognizing that postoperative events extend beyond the traditional 30-day window, recent studies have advocated for an extended observation period of 90 days to capture a more comprehensive spectrum of postoperative complications [ 35 , 36 , 37 , 38 , 39 ]. Specifically, the 90-day postoperative mortality metric has gained prominence as a robust measure of surgical quality, particularly for procedures involving the digestive tract or the head and neck [ 35 , 36 , 37 , 38 , 39 ]. Given the evolving understanding of the prolonged impact of surgery, we designated 90-day postoperative complications as a primary outcome in our study. This timeframe allows for a nuanced assessment of acute and subacute surgical complications, providing a more comprehensive perspective on patient outcomes. To maintain consistency with established practices and enhance comparability with prior research, we adhered to the definition of 30-day and 90-day in-hospital postoperative mortality as utilized in previous studies [ 27 , 29 , 30 , 31 , 32 , 35 , 36 , 37 , 38 , 39 ]. Consequently, patients who succumbed on the 91st day or later post-hospitalization were considered alive in our study, and those who died outside the hospital within 90 days were not included in the mortality outcome. In conclusion, the choice of assessing 30- and 90-day postoperative complications aligns with contemporary views on capturing the continuum of surgical outcomes, offering a more nuanced understanding of acute and subacute complications associated with the procedures under investigation.
A patient with sarcopenia receiving elective surgery is a patient with certain systemic imbalances and a worse biological reserve, which may contribute to a poor postoperative prognosis; this finding is consistent with a previous study finding [ 45 ]. Moreover, many risk factors are closely related to sarcopenia, for example, increasing age, malnutrition, alcoholism, smoking, insomnia, and chronic diseases, which often affect surgical prognosis and cause postoperative death [ 46 , 47 , 48 ]. Nevertheless, after matching for age, sex, income level, urbanization, coexisting medical conditions, hospital level, type of anesthesia, ASA score, and surgical type, sarcopenia is still an independent risk factor for 30-day and 90-day postoperative pneumonia, bleeding, septicemia, overall surgical complications, and mortality (Tables 2 and 3 ). In addition, not only the ORs of 30-day surgical complications and mortality but also the aORs of 90-day surgical complications and mortality were highly significant (Table 3 ; Fig. 2 ). The subacute surgical complications (90 d) may also be critical in patients with sarcopenia receiving surgery. Based on the outcomes of 30-day and 90-day surgical complications, patients with sarcopenia experience not only acute surgical complications but also subacute surgical complications after receiving elective surgery. The adverse outcomes of surgery in patients with sarcopenia do not alleviate even 30 days after surgery (Figs. 1 and 2 ).
The influence of sarcopenia on the prognosis of surgery is still unclear because of the small sample size, different definitions of sarcopenia, and different surgical types [ 10 , 11 , 13 , 14 , 15 , 16 , 49 , 50 , 51 , 52 , 53 , 54 , 55 ]. Thus far, no study with sufficient sample size or with appropriate matching has investigated the association of sarcopenia with 30-day and 90-day surgical complications and mortality after elective surgery. To the best of our knowledge, this is the first study to use the latest definition of sarcopenia based on ICD-10 and to demonstrate 30-day and 90-day adverse outcomes of surgery in patients with sarcopenia and nonsarcopenia receiving elective surgery. According to our literature review, studies have not compared 30-day and 90-day surgical complications between sarcopenia and nonsarcopenia groups. Our study is the first to demonstrate that patients with sarcopenia exhibited significantly increased rates of 30-day and 90-day adverse outcomes, including postoperative pneumonia, bleeding, septicemia, and mortality after elective surgery.
Among various adverse outcomes after major surgery, postoperative septicemia is one of the key factors leading to the death of patients with sarcopenia [ 56 , 57 , 58 , 59 ]. Our findings indicated that the incidence of 30-day and 90-day postoperative septicemia was significantly higher among patients with sarcopenia than among those without sarcopenia (Tables 2 and 3 ). The high incidence of postoperative septicemia in sarcopenia patients receiving surgery can be attributed to low immunity compared with that of nonsarcopenia patients [ 60 , 61 ]. Muscle fibers can produce cytokines and interleukins, inhibiting the secretion of tumor necrosis factor and mediating insulin resistance [ 62 , 63 ]. Sarcopenia reduces cellular immune function, increases the level of proinflammatory factors, and increases the possibility of infection in the body [ 60 , 61 ]. Moreover, the level of glutamine, which is an activator of lymphocytes and monocytes, is significantly reduced in patients with sarcopenia, thereby partly weakening their immunity [ 64 ]. Studies have suggested that sarcopenia may be one of the predictors of infection after colon cancer surgery [ 11 ].
Decreased immunity in patients with sarcopenia not only increases the possibility of postoperative infection but also increases the incidence of postoperative pneumonia [ 60 , 61 , 65 ]. In addition, patients with sarcopenia receiving surgery may experience difficulty in sputum removal and a high incidence of choking or aspiration pneumonia due to muscular weakness [ 66 , 67 ]. Soma et al. reported that preoperative sarcopenia in patients with esophageal cancer increases the risk of postoperative respiratory disease [ 68 ]; this is consistent with our findings. The increase in postoperative pneumonia may be related to the decrease in skeletal muscle mass and the weakening of respiratory and swallowing muscles in patients with sarcopenia [ 66 , 67 ]. Jain et al. demonstrated that short-term resistance exercise training and protein supplementation before surgery can increase the mass and strength of skeletal muscles and reduce fat content, thereby improving immunity and reducing the incidence of postoperative pulmonary complications [ 69 ]. Therefore, preoperative sarcopenia, swallowing function, and respiratory muscle training should be improved before elective surgery to decrease the incidence of postoperative pneumonia, other surgical complications, and mortality.
Our study discovered that patients with sarcopenia had a significantly increased incidence of 30-day and 90-day postoperative bleeding. To the best of our knowledge, no study has reported that sarcopenia directly alters the coagulation system; however, large retrospective studies have demonstrated that malnutrition can lead to postoperative bleeding in patients undergoing colorectal resection and pancreatic surgery, increase the risks of respiratory failure or infection, and even increase the mortality rate of patients [ 70 , 71 ].
The present study used data from the NHIRD, which reliably records the detailed medical information of Taiwanese patients, and this database has been used in many high-quality studies [ 17 , 20 , 21 , 27 , 28 ]. Furthermore, a large PSM-based design was employed in the comparative study to maintain balance among the confounders of the case and control groups—all in the absence of bias (Table 1 ). However, this study has a few limitations. First, PSM cannot control factors that are not accounted for in the model, and it is predicated on an explicit selection bias of the factors that can be matched. Second, because all patients were enrolled from an Asian population, the corresponding ethnic susceptibilities in non-Asian populations are unclear. However, no significant differences in the postoperative adverse outcomes and mortality have been reported between Asian and non-Asian populations; the results should be cautiously extrapolated to non-Asian populations. Third, another limitation of this study pertains to the diagnosis of sarcopenia, which relies solely on the availability of the ICD code. Consequently, if an individual is unintentionally omitted from receiving the sarcopenia code, they are categorized as not having sarcopenia. We acknowledge that this approach may result in potential underestimation. Recognizing this limitation, we emphasize the importance of conducting further prospective studies to yield more accurate and comprehensive results in this area.
We demonstrated that sarcopenia is an independent risk factor for 30-day and 90-day adverse postoperative outcomes such as postoperative pneumonia, bleeding, septicemia, and mortality after elective surgery. Therefore, preoperative sarcopenia, swallowing function, and respiratory muscle training should be corrected before elective surgery to reduce the incidence of postoperative complications that contribute to the decrease in surgical mortality.
Data availability
The datasets essential for supporting the conclusions of this study are provided within the manuscript and its supplementary files.
Abbreviations
Adjusted odds ratio
Confidence interval
International Classification of Diseases, Ninth Revision, Clinical Modification
International Classification of Diseases, Tenth Revision, Clinical Modification
Propensity score matching
National Health Insurance Research Database
American Society of Anesthesiology
Standard deviation
Standardized mean difference
Interquartile range
National Health Insurance
Skeletal muscle mass index
Cruz-Jentoft AJ, Bahat G, Bauer J, Boirie Y, Bruyere O, Cederholm T, Cooper C, Landi F, Rolland Y, Sayer AA, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. 2019;48(1):16–31.
Article PubMed Google Scholar
Choe HJ, Cho BL, Park YS, Roh E, Kim HJ, Lee SG, Kim BJ, Kim M, Won CW, Park KS, et al. Gender differences in risk factors for the 2 year development of Sarcopenia in community-dwelling older adults. J Cachexia Sarcopenia Muscle. 2022;13(3):1908–18.
Article PubMed PubMed Central Google Scholar
Chen X, Hou L, Zhang Y, Dong B. Analysis of the prevalence of Sarcopenia and its risk factors in the Elderly in the Chengdu Community. J Nutr Health Aging. 2021;25(5):600–5.
Article CAS PubMed Google Scholar
Hwang J, Park S. Gender-specific risk factors and prevalence for Sarcopenia among Community-Dwelling Young-Old adults. Int J Environ Res Public Health 2022, 19(12).
Ebadi M, Bhanji RA, Mazurak VC, Montano-Loza AJ. Sarcopenia in cirrhosis: from pathogenesis to interventions. J Gastroenterol. 2019;54(10):845–59.
Yin J, Lu X, Qian Z, Xu W, Zhou X. New insights into the pathogenesis and treatment of Sarcopenia in chronic heart failure. Theranostics. 2019;9(14):4019–29.
Article CAS PubMed PubMed Central Google Scholar
Janssen I. Influence of Sarcopenia on the development of physical disability: the Cardiovascular Health Study. J Am Geriatr Soc. 2006;54(1):56–62.
Lim JY, Frontera WR. Single skeletal muscle fiber mechanical properties: a muscle quality biomarker of human aging. Eur J Appl Physiol. 2022;122(6):1383–95.
Sindhar S, Kallogjeri D, Wildes TS, Avidan MS, Piccirillo JF. Association of Preoperative Functional Performance with outcomes after Surgical Treatment of Head and Neck Cancer: a clinical severity staging system. JAMA Otolaryngol Head Neck Surg. 2019;145(12):1128–36.
Sandini M, Patino M, Ferrone CR, Alvarez-Perez CA, Honselmann KC, Paiella S, Catania M, Riva L, Tedesco G, Casolino R, et al. Association between changes in body composition and Neoadjuvant Treatment for Pancreatic Cancer. JAMA Surg. 2018;153(9):809–15.
Feliciano EMC, Kroenke CH, Meyerhardt JA, Prado CM, Bradshaw PT, Kwan ML, Xiao J, Alexeeff S, Corley D, Weltzien E, et al. Association of Systemic Inflammation and Sarcopenia with Survival in Nonmetastatic Colorectal Cancer: results from the C SCANS study. JAMA Oncol. 2017;3(12):e172319.
Friedman J, Lussiez A, Sullivan J, Wang S, Englesbe M. Implications of Sarcopenia in major surgery. Nutr Clin Pract. 2015;30(2):175–9.
Wang H, Yang R, Xu J, Fang K, Abdelrahim M, Chang L. Sarcopenia as a predictor of postoperative risk of complications, mortality and length of stay following gastrointestinal oncological surgery. Ann R Coll Surg Engl. 2021;103(9):630–7.
Hendrickson NR, Mayo Z, Shamrock A, Kesler K, Glass N, Nau P, Miller BJ. Sarcopenia is associated with increased mortality but not complications following resection and reconstruction of sarcoma of the extremities. J Surg Oncol. 2020;121(8):1241–8.
Kim EY, Lee HY, Kim KW, Lee JI, Kim YS, Choi WJ, Kim JH. Preoperative computed tomography-determined Sarcopenia and Postoperative Outcome after surgery for Non-small Cell Lung Cancer. Scand J Surg. 2018;107(3):244–51.
Siegal SR, Dolan JP, Dewey EN, Guimaraes AR, Tieu BH, Schipper PH, Hunter JG. Sarcopenia is not associated with morbidity, mortality, or recurrence after esophagectomy for cancer. Am J Surg. 2018;215(5):813–7.
Sun MY, Chang CL, Lu CY, Wu SY, Zhang JQ. Sarcopenia as an independent risk factor for specific cancers: a propensity score-matched Asian Population-based Cohort Study. Nutrients 2022, 14(9).
Huang YM, Chen WM, Chen M, Shia BC, Wu SY. Sarcopenia is an independent risk factor for severe Diabetic Nephropathy in Type 2 diabetes: a long-term Follow-Up propensity score-matched diabetes cohort study. J Clin Med 2022, 11(11).
Tsai YH, Chen WM, Chen MC, Shia BC, Wu SY, Huang CC. Effect of Pre-Existing Sarcopenia on Oncological Outcomes for Oral Cavity Squamous Cell Carcinoma Undergoing Curative Surgery: A Propensity Score-Matched, Nationwide, Population-Based Cohort Study. Cancers (Basel) 2022, 14(13).
Sun M, Chang CL, Lu CY, Zhang J, Wu SY. Effect of opioids on cancer survival in patients with chronic pain: a propensity score-matched population-based cohort study. Br J Anaesth. 2022;128(4):708–17.
Sun M, Lin JA, Chang CL, Wu SY, Zhang J. Association between long-term opioid use and cancer risk in patients with chronic pain: a propensity score-matched cohort study. Br J Anaesth. 2022;129(1):84–91.
Bijlsma AY, Meskers CG, Ling CH, Narici M, Kurrle SE, Cameron ID, Westendorp RG, Maier AB. Defining Sarcopenia: the impact of different diagnostic criteria on the prevalence of Sarcopenia in a large middle aged cohort. Age (Dordr). 2013;35(3):871–81.
Anker SD, Morley JE, von Haehling S. Welcome to the ICD-10 code for Sarcopenia. J Cachexia Sarcopenia Muscle. 2016;7(5):512–4.
Chien MY, Huang TY, Wu YT. Prevalence of Sarcopenia estimated using a bioelectrical impedance analysis prediction equation in community-dwelling elderly people in Taiwan. J Am Geriatr Soc. 2008;56(9):1710–5.
Wang S, Xie H, Gong Y, Kuang J, Yan L, Ruan G, Gao F, Gan J. The value of L3 skeletal muscle index in evaluating preoperative nutritional risk and long-term prognosis in colorectal cancer patients. Sci Rep. 2020;10(1):8153.
Austin PC. Optimal caliper widths for propensity-score matching when estimating differences in means and differences in proportions in observational studies. Pharm Stat. 2011;10(2):150–61.
Lin JA, Liao CC, Chang CC, Chang H, Chen TL. Postoperative adverse outcomes in intellectually disabled surgical patients: a nationwide population-based study. PLoS ONE. 2011;6(10):e26977.
Lin JA, Liao CC, Lee YJ, Wu CH, Huang WQ, Chen TL. Adverse outcomes after major surgery in patients with systemic lupus erythematosus: a nationwide population-based study. Ann Rheum Dis. 2014;73(9):1646–51.
Liao CC, Shen WW, Chang CC, Chang H, Chen TL. Surgical adverse outcomes in patients with schizophrenia: a population-based study. Ann Surg. 2013;257(3):433–8.
Ghaferi AA, Birkmeyer JD, Dimick JB. Variation in hospital mortality associated with inpatient surgery. N Engl J Med. 2009;361(14):1368–75.
Khuri SF, Henderson WG, DePalma RG, Mosca C, Healey NA, Kumbhani DJ. Participants in the VANSQIP: determinants of long-term survival after major surgery and the adverse effect of postoperative complications. Ann Surg. 2005;242(3):326–41. discussion 341 – 323.
Chang CC, Hu CJ, Lam F, Chang H, Liao CC, Chen TL. Postoperative adverse outcomes in surgical patients with epilepsy: a population-based study. Epilepsia. 2012;53(6):987–94.
Austin PC. The performance of different propensity score methods for estimating marginal hazard ratios. Stat Med. 2013;32(16):2837–49.
Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240(2):205–13.
Qin L, Chen TM, Kao YW, Lin KC, Yuan KS, Wu ATH, Shia BC, Wu SY. Predicting 90-Day mortality in Locoregionally Advanced Head and Neck Squamous Cell Carcinoma after curative surgery. Cancers (Basel) 2018, 10(10).
Lin KC, Chen TM, Yuan KS, Wu ATH, Wu SY. Assessment of Predictive Scoring System for 90-Day mortality among patients with locally Advanced Head and Neck squamous cell Carcinoma who have completed concurrent chemoradiotherapy. JAMA Netw Open. 2020;3(3):e1920671.
Shia BC, Qin L, Lin KC, Fang CY, Tsai LL, Kao YW, Wu SY. Age comorbidity scores as risk factors for 90-day mortality in patients with a pancreatic head adenocarcinoma receiving a pancreaticoduodenectomy: a National Population-based study. Cancer Med. 2020;9(2):562–74.
Pugalenthi A, Protic M, Gonen M, Kingham TP, Angelica MI, Dematteo RP, Fong Y, Jarnagin WR, Allen PJ. Postoperative complications and overall survival after pancreaticoduodenectomy for pancreatic ductal adenocarcinoma. J Surg Oncol. 2016;113(2):188–93.
Mise Y, Vauthey JN, Zimmitti G, Parker NH, Conrad C, Aloia TA, Lee JE, Fleming JB, Katz MH. Ninety-day postoperative mortality is a legitimate measure of Hepatopancreatobiliary Surgical Quality. Ann Surg. 2015;262(6):1071–8.
Lieffers JR, Bathe OF, Fassbender K, Winget M, Baracos VE. Sarcopenia is associated with postoperative infection and delayed recovery from colorectal cancer resection surgery. Br J Cancer. 2012;107(6):931–6.
Yang TR, Luo K, Deng X, Xu L, Wang RR, Ji P, Brittany, Park, et al. Consensus-defined Sarcopenia predicts adverse outcomes after elective abdominal surgery: meta-analysis. World J Emerg Surg. 2022;17(1):36.
Lobo DN, Gianotti L, Adiamah A, Barazzoni R, Deutz NEP, Dhatariya K, Greenhaff PL, Hiesmayr M, Hjort Jakobsen D, Klek S, et al. Perioperative nutrition: recommendations from the ESPEN expert group. Clin Nutr. 2020;39(11):3211–27.
Ansaripour A, Arjomandi Rad A, Koulouroudias M, Angouras D, Athanasiou T, Kourliouros A. Sarcopenia adversely affects outcomes following cardiac surgery: a systematic review and Meta-analysis. J Clin Med 2023, 12(17).
Park B, Bhat S, Xia W, Barazanchi AWH, Frampton C, Hill AG, MacCormick AD. Consensus-defined Sarcopenia predicts adverse outcomes after elective abdominal surgery: meta-analysis. BJS Open 2023, 7(4).
Shen Y, Hao Q, Zhou J, Dong B. The impact of frailty and sarcopenia on postoperative outcomes in older patients undergoing gastrectomy surgery: a systematic review and meta-analysis. BMC Geriatr. 2017;17(1):188.
Wahlen BM, Mekkodathil A, Al-Thani H, El-Menyar A. Impact of Sarcopenia in trauma and surgical patient population: a literature review. Asian J Surg. 2020;43(6):647–53.
Roubenoff R. Sarcopenia and its implications for the elderly. Eur J Clin Nutr. 2000;54(Suppl 3):S40–47.
Yuan H, Goto N, Akita H, Shiraishi N, He HJ. Morphometric analysis of the human cervical motoneurons in the aging process. Okajimas Folia Anat Jpn. 2000;77(1):1–4.
Hirase T, Haghshenas V, Bratescu R, Dong D, Kuo PH, Rashid A, Kavuri V, Hanson DS, Meyer BC, Marco RAW. Sarcopenia predicts perioperative adverse events following complex revision surgery for the thoracolumbar spine. Spine J. 2021;21(6):1001–9.
Flexman AM, Street J, Charest-Morin R. The impact of frailty and sarcopenia on patient outcomes after complex spine surgery. Curr Opin Anaesthesiol. 2019;32(5):609–15.
Charest-Morin R, Street J, Zhang H, Roughead T, Ailon T, Boyd M, Dvorak M, Kwon B, Paquette S, Dea N, et al. Frailty and Sarcopenia do not predict adverse events in an elderly population undergoing non-complex primary elective surgery for degenerative conditions of the lumbar spine. Spine J. 2018;18(2):245–54.
Yamashita S, Iguchi T, Koike H, Wakamiya T, Kikkawa K, Kohjimoto Y, Hara I. Impact of preoperative Sarcopenia and myosteatosis on prognosis after radical cystectomy in patients with bladder cancer. Int J Urol. 2021;28(7):757–62.
Kobayashi A, Kaido T, Hamaguchi Y, Okumura S, Shirai H, Yao S, Kamo N, Yagi S, Taura K, Okajima H, et al. Impact of sarcopenic obesity on outcomes in patients undergoing hepatectomy for Hepatocellular Carcinoma. Ann Surg. 2019;269(5):924–31.
Antoniou GA, Rojoa D, Antoniou SA, Alfahad A, Torella F, Juszczak MT. Effect of low skeletal muscle Mass on post-operative survival of patients with abdominal aortic aneurysm: a prognostic factor review and Meta-analysis of Time-to-Event Data. Eur J Vasc Endovasc Surg. 2019;58(2):190–8.
Stone L, Olson B, Mowery A, Krasnow S, Jiang A, Li R, Schindler J, Wax MK, Andersen P, Marks D, et al. Association between Sarcopenia and Mortality in patients undergoing Surgical Excision of Head and Neck Cancer. JAMA Otolaryngol Head Neck Surg. 2019;145(7):647–54.
Mokart D, Giaoui E, Barbier L, Lambert J, Sannini A, Chow-Chine L, Brun JP, Faucher M, Guiramand J, Ewald J, et al. Postoperative sepsis in cancer patients undergoing major elective digestive surgery is associated with increased long-term mortality. J Crit Care. 2016;31(1):48–53.
Ou L, Chen J, Hillman K, Flabouris A, Parr M, Assareh H, Bellomo R. The impact of post-operative sepsis on mortality after hospital discharge among elective surgical patients: a population-based cohort study. Crit Care. 2017;21(1):34.
Chen PY, Luo CW, Chen MH, Yang ML, Kuan YH. Epidemiological characteristics of postoperative Sepsis. Open Med (Wars). 2019;14:928–38.
Flanagan JM, Read C, Shindul-Rothschild J. Factors Associated with the rate of Sepsis after surgery. Crit Care Nurse. 2020;40(5):e1–9.
Lutz CT, Quinn LS. Sarcopenia, obesity, and natural killer cell immune senescence in aging: altered cytokine levels as a common mechanism. Aging. 2012;4(8):535–46.
Rong YD, Bian AL, Hu HY, Ma Y, Zhou XZ. Study on relationship between elderly Sarcopenia and inflammatory cytokine IL-6, anti-inflammatory cytokine IL-10. BMC Geriatr. 2018;18(1):308.
Pedersen BK, Febbraio MA. Muscle as an endocrine organ: focus on muscle-derived interleukin-6. Physiol Rev. 2008;88(4):1379–406.
Imierska M, Kurianiuk A, Blachnio-Zabielska A. The influence of physical activity on the bioactive lipids metabolism in obesity-Induced muscle insulin resistance. Biomolecules 2020, 10(12).
Andrews FJ, Griffiths RD. Glutamine: essential for immune nutrition in the critically ill. Br J Nutr. 2002;87(Suppl 1):S3–8.
Torrance HDT, Longbottom ER, Vivian ME, Lalabekyan B, Abbott TEF, Ackland GL, Hinds CJ, Pearse RM, O’Dwyer MJ. Post-operative immune suppression is mediated via reversible, Interleukin-10 dependent pathways in circulating monocytes following major abdominal surgery. PLoS ONE. 2018;13(9):e0203795.
Okazaki T, Ebihara S, Mori T, Izumi S, Ebihara T. Association between Sarcopenia and pneumonia in older people. Geriatr Gerontol Int. 2020;20(1):7–13.
Ebihara S, Sekiya H, Miyagi M, Ebihara T, Okazaki T. Dysphagia, dystussia, and aspiration pneumonia in elderly people. J Thorac Dis. 2016;8(3):632–9.
Soma D, Kawamura YI, Yamashita S, Wake H, Nohara K, Yamada K, Kokudo N. Sarcopenia, the depletion of muscle mass, an independent predictor of respiratory complications after oncological esophagectomy. Dis Esophagus 2019, 32(3).
Jain R, Handorf E, Khare V, Blau M, Chertock Y, Hall MJ. Impact of Baseline Nutrition and Exercise Status on Toxicity and outcomes in Phase I and II oncology clinical trial participants. Oncologist. 2020;25(2):161–9.
Lee DU, Fan GH, Hastie DJ, Addonizio EA, Suh J, Prakasam VN, Karagozian R. The clinical impact of malnutrition on the postoperative outcomes of patients undergoing colorectal resection surgery for colon or rectal cancer: propensity score matched analysis of 2011–2017 US hospitals. Surg Oncol. 2021;38:101587.
Lee DU, Hastie DJ, Fan GH, Addonizio EA, Lee KJ, Han J, Karagozian R. Effect of malnutrition on the postoperative outcomes of patients undergoing pancreatectomy for pancreatic cancer: Propensity score-matched analysis of 2011–2017 US hospitals. Nutr Clin Pract. 2022;37(1):117–29.
Download references
The work of Szu-Yuan Wu is supported by the Lo-Hsu Medical Foundation, Lotung Poh-Ai Hospital, under funding numbers 11001, 11010, 11013, and 11103 and the work of Jiaqiang Zhang is supported by the National Key Research and Development Program of China,under funding number 2023YFC2506903.
Author information
Yitian Yang and Mingyang Sun have contributed equally to this study (joint primary authors).
Szu-Yuan Wu and Jiaqiang Zhang have contributed equally to this study (joint Correspondence authors).
Authors and Affiliations
Department of Anesthesiology and Perioperative Medicine, Henan Provincial People’s Hospital, People’s Hospital of Zhengzhou University, Zhengzhou, China
Yitian Yang, Mingyang Sun & Jiaqiang Zhang
Graduate Institute of Business Administration, College of Management, Fu Jen Catholic University, Taipei, Taiwan
Wan-Ming Chen & Szu-Yuan Wu
Artificial Intelligence Development Center, Fu Jen Catholic University, Taipei, Taiwan
Department of Food Nutrition and Health Biotechnology, College of Medical and Health Science, Asia University, Taichung, Taiwan
Szu-Yuan Wu
Big Data Center, Lo-Hsu Medical Foundation, Lotung Poh-Ai Hospital, Yilan, Taiwan
Division of Radiation Oncology, Lo-Hsu Medical Foundation, Lotung Poh-Ai Hospital, Yilan, Taiwan
Department of Healthcare Administration, College of Medical and Health Science, Asia University, Taichung, Taiwan
Cancer Center, Lo-Hsu Medical Foundation, Lotung Poh-Ai Hospital, Yilan, Taiwan
Centers for Regional Anesthesia and Pain Medicine, Taipei Municipal Wan Fang Hospital, Taipei Medical University, Taipei, Taiwan
Department of Management, College of Management, Fo Guang University, Yilan, Taiwan
You can also search for this author in PubMed Google Scholar
Contributions
The collaborative effort of the authors resulted in the conception and design of the study, led by Yitian Yang, Mingyang Sun, Wan-Ming Chen, Szu-Yuan Wu, and Jiaqiang Zhang. Financial support for this work was provided by the Lo-Hsu Medical Foundation, Lotung Poh-Ai Hospital, with funding numbers 11001, 11010, 11013, and 11103, benefiting the research of Szu-Yuan Wu. The comprehensive collection and assembly of data were carried out by Yitian Yang, Szu-Yuan Wu, and Jiaqiang Zhang. The crucial tasks of data analysis and interpretation were undertaken by Jiaqiang Zhang and Szu-Yuan Wu. Administrative support was provided by Szu-Yuan Wu. The manuscript itself was written collaboratively by Yitian Yang, Mingyang Sun, Wan-Ming Chen, Szu-Yuan Wu, and Jiaqiang Zhang. Lastly, the final approval of the manuscript was granted by all authors, reflecting their unified contributions and dedication to the study’s completion.
Corresponding authors
Correspondence to Szu-Yuan Wu or Jiaqiang Zhang .
Ethics declarations
Competing interests.
The authors, Yitian Yang, Mingyang Sun, Wan-Ming Chen, Szu-Yuan Wu, and Jiaqiang Zhang, declare no potential conflicts of interest in relation to the research, its execution, or its publication.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
Rights and permissions.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Yang, Y., Sun, M., Chen, WM. et al. Adverse postoperative outcomes in elderly patients with sarcopenia. BMC Geriatr 24 , 561 (2024). https://doi.org/10.1186/s12877-024-05066-2
Download citation
Received : 19 August 2023
Accepted : 10 May 2024
Published : 27 June 2024
DOI : https://doi.org/10.1186/s12877-024-05066-2
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
The incidence of recurrent hernia after radical resection of prostate cancer is high, so this article discusses the incidence and risk factors of inguinal hernia after radical resection of prostate cancer.
This case control study was conducted in The First People’s Hospital of Huzhou clinical data of 251 cases underwent radical resection of prostate cancer in this hospital from March 2019 to May 2021 were retrospectively analyzed. According to the occurrence of inguinal hernia, the subjects were divided into study group and control group, and the clinical data of each group were statistically analyzed, Multivariate Logistic analysis was performed to find independent influencing factors for predicting the occurrence of inguinal hernia. The Kaplan-Meier survival curve was drawn according to the occurrence and time of inguinal hernia.
The overall incidence of inguinal hernia after prostate cancer surgery was 14.7% (37/251), and the mean time was 8.58 ± 4.12 months. The average time of inguinal hernia in patients who received lymph node dissection was 7.61 ± 4.05 (month), and that in patients who did not receive lymph node dissection was 9.16 ± 4.15 (month), and there was no significant difference between them ( P > 0.05). There were no statistically significant differences in the incidence of inguinal hernia with age, BMI, hypertension, diabetes, PSA, previous abdominal operations and operative approach ( P > 0.05), but there were statistically significant differences with surgical method and pelvic lymph node dissection ( P < 0.05). The incidence of pelvic lymph node dissection in the inguinal hernia group was 24.3% (14/57), which was significantly higher than that in the control group 11.8% (23/194). Logistic regression analysis showed that pelvic lymph node dissection was a risk factor for inguinal hernia after prostate cancer surgery (OR = 0.413, 95%Cl: 0.196–0.869, P = 0.02). Kaplan-Meier survival curve showed that the rate of inguinal hernia in the group receiving pelvic lymph node dissection was significantly higher than that in the control group ( P < 0.05).
Pelvic lymph node dissection is a risk factor for inguinal hernia after radical resection of prostate cancer.
Peer Review reports
Prostate cancer is a common malignant tumor in urology, which occurs in the prostate epithelial tissue, There are an average of 190,000 new cases of prostate cancer each year and about 80,000 deaths worldwide each year [ 1 , 2 ]. In recent years, the incidence of prostate cancer has increased year by year, seriously affecting the health and quality of life of patients [ 3 ]. Worldwide, the incidence of prostate cancer is second only to lung cancer, and its death rate ranks 7th among male cancer causes [ 4 ]. Radical resection of prostate cancer (RP) is the main means for the treatment of prostate cancer, and the surgical methods are generally divided into open radical resection of prostate cancer (RRP) and minimally invasive radical resection of prostate cancer, the latter including laparoscopic radical resection of prostate cancer (LRP) and robot-assisted laparoscopic radical resection of prostate cancer (RALP) [ 5 , 6 , 7 ].
Inguinal hernia (IH) is a relatively common disease in clinic, which is caused by increased abdominal pressure, thinning of abdominal wall, and bulging of abdominal organs. Inguinal hernias include direct hernias, oblique hernias and femoral hernias [ 8 ]. At the onset, lumps protruding outward from the inguinal region can be seen. If the intestines cannot return to the abdominal cavity in time, it is easy to cause intestinal necrosis, intestinal obstruction, intestinal perforation and other complications, which may endanger the life safety of patients in severe cases [ 9 , 10 ].
With the extensive development of radical resection of prostate cancer in various hospitals, the problem of postoperative inguinal hernia has gradually attracted the attention of urologists. The previously reported incidence of IH after radical prostate cancer surgery was approximately 13.7% [ 11 ]. A study by Nagatani S et al. showed that the incidence of inguinal hernia after radical prostate cancer surgery was 7-21%, most of which occurred within 2 years after surgery [ 12 ]. A study by Stranne J et al. showed that the cumulative risk of IH occurrence within 48 months in open radical resection for prostate cancer group and non-surgical group was 12.2% and 5.8%, respectively [ 13 ]. Most cases of IH require surgery due to pain, discomfort, and incarceration and are considered an advanced complication of radical resection of prostate cancer. The adhesion after radical resection of prostate cancer also increases the difficulty of hernia repair. Therefore, urologists need to be concerned not only about the risk of urinary incontinence and erectile dysfunction after radical resection of prostate cancer, but also about the occurrence of IH.
In recent 10 years, many scholars around the world have studied the risk factors of inguinal hernia after radical prostate cancer surgery. Currently, most of the studies believe that anastomotic stenosis, previous history of inguinal hernia, and patent processus vaginalis are risk factors, However there is no consensus on the risk of lymph node dissection. For example, Niitsu H et al. believed that pelvic lymph node dissection during radical prostate cancer operation might damage the pectineal foramina, thereby increasing the risk of inguinal hernia [ 14 ]. Contrary to the results of Johan Stranne’s study, the author suggested that previous incidence of inguinal hernia and advanced age increased the risk of inguinal hernia after radical prostate cancer surgery, and pelvic lymph node dissection was not a significant risk factor [ 15 ]. There is also no consistent conclusion on the influence of BMI, age and surgical method.
Therefore, in order to further investigate the risk factors of inguinal hernia after radical prostate cancer surgery, especially the correlation between pelvic lymph node dissection and inguinal hernia, this study was conducted. This study retrospectively analyzed the clinical data of 251 patients who underwent radical resection of prostate cancer in our hospital from March 2019 to May 2021, and investigated the risk factors of postoperative inguinal hernia. It is reported as follows:
Research objectives
The objective of this study was to explore the incidence and risk factors of inguinal hernia after radical resection of prostate cancer, which provides reference for further research and guide the clinician to choose the appropriate surgical method according to the patient’s condition.
Research methods
The patient was also examined by B-ultrasound every 3 months at the outpatient PSA review to verify the occurrence of inguinal hernia. The subjects were divided into the inguinal hernia group (study group) and the non-inguinal hernia group (control group), If the diagnosis of inguinal hernia occurred, the follow-up was completed, and the type and time of inguinal hernia were recorded; otherwise, the follow-up was 2 years, and the relevant clinical parameters of each group were statistically analyzed (age, BMI, hypertension, diabetes mellitus, PSA value, previous abdominal operations, operation methods, operative approach, pelvic lymph node dissection)and the correlation between these parameters and the occurrence of inguinal hernia was analyzed, and the risk factors of inguinal hernia were found by Logistic regression analysis. According to the occurrence and time of inguinal hernia, Kaplan-Meier survival curve was drawn to compare the differences between the two groups.
The content of this study has been approved by the Ethics Committee of our hospital(approval number, 2,018,137). All patients signed informed consent forms. This is the protocol was registered on the Chinese Clinical Trial Registry. The study is planned to begin in mid-March 2019 and is planned to end by May 2021.
Inclusion criteria
Patients who received radical surgery for prostate cancer in Huzhou First People’s Hospital from March 2019 to May 2021; PSA was reviewed every 3 months after surgery, and check the inguinal area for protruding masses. Complete the 2-year follow-up plan.
Exclusion criteria
Patients with inguinal hernia before operation; patients with prior inguinal hernia surgery.
Statistical methods
SPSS 21.0 statistical software was used for statistical processing, the research data followed normal distribution, and the measured data were represented by X ± S. P < 0.05 was considered statistically significant.
From March 2019 to May 2021, 318 cases of radical prostatectomy were performed in our hospital, during the follow-up period, a total of 28 cases died of other diseases, a total of 39 cases were lost to follow-up or clinical data were incomplete, and a total of 251 cases were finally followed up. There were no significant differences in age, BMI, hypertension, diabetes, PSA, previous abdominal operations and operative approach between the two groups ( P > 0.05), while there were significant differences in surgical method and pelvic lymph node dissection ( P < 0.05). The incidence of pelvic lymph node dissection in the inguinal hernia group 24.3% (14/57) was significantly higher than that in the control group 11.8% (23/194). See Table 1 for details.
Multivariate Logistic regression analysis of risk factors showed that pelvic lymph node dissection was a risk factor for inguinal hernia after prostate cancer surgery (OR =0.413, 95%Cl: 0.196-0.869, P = 0.02). There was no statistical significance in age, BMI, hypertension, diabetes, PSA value, previous abdominal operations, operation method, operative approach were not risk factors for inguinal hernia ( P > 0.05). See Table 2 for details.
The cases of inguinal hernia were grouped according to whether or not they had received pelvic lymph node dissection. The incidence and time of inguinal hernia in the two groups were recorded, and the Kaplan-Meier survival curve was drawn. The overall incidence of inguinal hernia after radical resection of prostate cancer was 14.7% (37/251), There were 26 cases with indirect hernia, accounting for 70.2% (26/37), 21.6% (8/37) with direct hernia, 8.2% (3/37) with oblique hernia and direct hernia, and the mean time of occurrence was 8.58 ± 4.12 months. The average time of inguinal hernia was 7.61 ± 4.05 (month) for those who received lymph node dissection and 9.16 ± 4.15 (month) for those who did not receive lymph node dissection, and there was no significant difference between them ( P > 0.05). The incidence of inguinal hernia in the group receiving pelvic lymph node dissection was significantly higher than that in the control group ( P < 0.05). See Fig. 1 for details.
Survival curve of pelvic lymph node dissection and inguinal hernia (month)
In recent years, the incidence of prostate cancer has increased year by year, seriously affecting the health and quality of life of patients, the complications after radical prostate cancer surgery mainly include urinary incontinence and sexual dysfunction, but inguinal hernia is also one of the common complications [ 16 ]. Liu L et al. found that open radical resection for prostate cancer technique and advanced patient age, especially those over 80 years old, are associated with a higher incidence of IH. Appropriate prophylaxis during surgery should be evaluated in high-risk patients [ 17 ].In some regional studies, low BMI has been identified as a risk factor for IH, and the risk threshold for BMI has not been determined, which is about BMI < 25 kg/m2 [ 18 ]. However, a number of studies have found that low BMI does not increase the risk of postoperative IH [ 19 , 20 ]. At present, there is no uniform conclusion on the risk of IH between open radical resection for prostate cancer and laparoscopic radical prostatectomy. The study of Alder R scholars believed that the incidence of IH after laparoscopic radical prostatectomy was relatively low [ 21 ], while Otaki T’s study shows that the incidence of IH after laparoscopic radical prostatectomy is 7.3% and that of open radical resection for prostate cancer is 8.4%, showing no statistical difference between them [ 20 ]. There is no consensus on whether pelvic lymph node dissection is a risk factor for inguinal hernia [ 14 , 15 ]. In short, the specific mechanism of inguinal hernia after radical prostate cancer surgery is unclear.
This study retrospectively analyzed the clinical data of 251 cases treated in our hospital, and found that the overall incidence of inguinal hernia was 14.7% (37/251), which was consistent with most of the current research results. We also found that the average time of occurrence of inguinal hernia after surgery was 8.58 ± 4.12 months, which provided certain guidance for our postoperative follow-up time.
In this study, through Logistic multivariate analysis, it was found that pelvic lymph node dissection was a risk factor for inguinal hernia after prostate cancer surgery (OR = 0.413, 95%Cl: 0.196–0.869, P = 0.02). There was no statistical significance in age, BMI, hypertension, diabetes, PSA value, previous abdominal operations, operation method, operative approach and the occurrence of inguinal hernia after prostate cancer surgery ( P > 0.05),but there were statistically significant differences with surgical method and pelvic lymph node dissection ( P < 0.05). Therefore, the advantages and disadvantages of pelvic lymph node dissection should be reasonably evaluated for low-medium-risk prostate cancer patients, so as to avoid the occurrence of inguinal hernia. By drawing Kaplan-Meier survival curve, it was found that the rate of inguinal hernia in the group receiving pelvic lymph node dissection was significantly higher than that in the control group. Some studies believe that pelvic lymph node dissection during radical resection of prostate cancer operation will cause postoperative scar contraction in the inguinal region, resulting in an increase in abdominal pressure outward and downward, resulting in an increase in the incidence of inguinal hernia. Lodding P designed a comparative study between the group of radical resection of prostate cancer plus pelvic lymph node dissection, the group of pelvic lymph node dissection and the group without operation. They found that the incidence of inguinal hernia in the three observation groups was 13.6%, 7.6% and 3.1%, respectively, and the difference between the prostatectomy group and the group without operation was statistically significant. There was no significant difference between the group and pelvic lymph node dissection group. This result implies that pelvic lymph node dissection is an important factor in the development of inguinal hernia [ 22 ]. Another Sun M study compared the incidence of inguinal hernias after radical prostate cancer surgery and pelvic lymph node dissection alone, and showed that the risk of inguinal hernias increased by 6.8% and 7.8% at 5 and 10 years, respectively, in the radical prostate cancer resection group compared with the pelvic lymph node dissection group [ 23 ]. Niitsu H et al. believed that pelvic lymph node dissection during radical resection of prostate cancer might damage the pectineal foramina, while inguinal hernia originated from the defective pectineal foramina [ 14 ].
Shimbo M et al. found that due to prostatectomy and vesicourethral anastomosis, preoperative and postoperative sagittal MRI images showed that the rectovesical excavation (RE) was moved downward by about 2 to 3 cm [ 24 ]. Accordingly, they speculated that due to the displacement of RE, the peritoneum and vas deferens after urethrovesical anastomosis were pulled, which further pulled the opening of the inner ring and caused it to shift medially, which led to the occurrence of postoperative IH. Based on this theory, many scholars have prevented the occurrence of hernia after operation by reducing the tension of peritoneum and vas deferens at the inner ring and ligation and rupture of sheathing process. Several other articles have reported the role of preserving the retropubic space (RS) in preventing IH after radical resection of prostate cancer. Chang KD et al. found that robot-assisted laparoscopic radical prostatectomywith retained Retzius space significantly reduced the incidence of postoperative IH compared with standard robot-assisted laparoscopic radical prostatectomy [ 25 ]. In addition, the study of Matsubara et al. also showed that compared with standard open radical resection for prostate cancer, the incidence of IH after transperineal radical resection of prostate cancer with retained anatomical structures such as the Retzius space was lower [ 26 ]. Therefore, urological surgeons can take some effective measures in the operation to prevent the recurrence of inguinal hernia.
In this study, we identified risk factors for inguinal hernia after pelvic lymphadenectomy for prostate cancer. Other risk factors such as age, BMI, hypertension, diabetes mellitus, PSA value, history of abdominal surgery, operative method, operative approach were not significant in multivariate analysis, which was inconsistent with the results of Iwamoto H et al [ 27 ]. They found that dilatation of the right internal inguinal ring and different manipulation of the medial peritoneal incision of the ventral femoral ring were independent risk factors for IH after laparoscopic radical prostatectomy. The reason why postoperative IH occurs more often on the right side is not known. Alder R et al. found that the incidence of IH after open radical prostate cancer treatment was significantly higher than laparoscopic radical prostate cancer treatment [ 21 ], but our study did not show a difference between the two groups, possibly due to the small number of cases included in open radical prostate surgery.
In summary, the incidence of inguinal hernia after radical prostate cancer surgery is relatively high, and the specific cause is still unclear. Our study shows that pelvic lymph node dissection is a risk factor for inguinal hernia.
Limitations
The sample size of this study is small, and it belongs to a single-center study, so the representativeness of the research conclusions may not be strong. This time, we followed up the samples for 2 years, which was not long enough and may have overlooked the real incidence of inguinal hernia. In addition, this study is a retrospective study, and the clinical parameters observed are not very comprehensive, which may ignore the influence of other factors on the IH. Because our data is derived from clinical data, some data cannot be detected. These problems need further study by more scholars.
Data availability
We cannot provide and share our datasets in publicly available repositories because of informed consent for participants as confidential patient data. Data may be obtained from the corresponding author upon reasonable request.
Sekhoacha M, Riet K, Motloung P et al. Prostate Cancer Review: Genetics, diagnosis, Treatment options, and alternative approaches. Molecules 2022; 27.
Rawla P. Epidemiology of prostate Cancer. World J Oncol. 2019;10(2):63–89.
Article CAS PubMed PubMed Central Google Scholar
Vietri MT, D’Elia G, Caliendo G et al. Hereditary prostate Cancer: genes related, Target Therapy and Prevention. Int J Mol Sci 2021; 22.
Williams IS, McVey A, Perera S, et al. Modern paradigms for prostate cancer detection and management. Med J Aust. 2022;217:424–33.
Article PubMed PubMed Central Google Scholar
Achard V, Panje CM, Engeler D, et al. Localized Local Adv Prostate Cancer: Treat Options Oncol. 2021;99:413–21.
CAS Google Scholar
Davis M, Egan J, Marhamati S, et al. Retzius-Sparing Robot-assisted robotic prostatectomy: past, Present, and Future. Urol Clin North Am. 2021;48:11–23.
Article PubMed Google Scholar
Heidenreich A, Pfister D. Radical cytoreductive prostatectomy in men with prostate cancer and oligometastatic disease. Curr Opin Urol. 2020;30:90–7.
Miller HJ. Inguinal hernia: mastering the anatomy. Surg Clin North Am. 2018;98:607–21.
Gamborg S, Marcussen ML, Öberg S, Rosenberg J. Inguinal hernia repair but no Hernia Present: a Nationwide Cohort Study. Surg Technol Int. 2022;40:171–4.
PubMed Google Scholar
Chien S, Cunningham D, Khan KS. Inguinal hernia repair: a systematic analysis of online patient information using the modified ensuring Quality Information for patients tool. Ann R Coll Surg Engl. 2022;104:242–8.
CAS PubMed PubMed Central Google Scholar
Perez AJ, Campbell S. Inguinal hernia repair in older persons. J Am Med Dir Assoc. 2022;23(4):563–7.
Nagatani S, Tsumura H, Kanehiro T, et al. Inguinal hernia associated with radical prostatectomy. Surg Today. 2021;51:792–7.
Stranne J, Johansson E, Nilsson A, et al. Inguinal hernia after radical prostatectomy for prostate cancer: results from a randomized setting and a nonrandomized setting. Eur Urol. 2010;58:719–26.
Niitsu H, Taomoto J, Mita K, et al. Inguinal hernia repair with the mesh plug method is safe after radical retropubic prostatectomy. Surg Today. 2014;44:897–901.
Stranne J, Hugosson J, Lodding P. Post-radical retropubic prostatectomy inguinal hernia: an analysis of risk factors with special reference to preoperative inguinal hernia morbidity and pelvic lymph node dissection. J Urol. 2006;176:2072–6.
Tolle J, Knipper S, Pose R, et al. Evaluation of risk factors for adverse functional outcomes after Radical Prostatectomy in patients with previous transurethral surgery of the prostate. Urol Int. 2021;105:408–13.
Liu L, Xu H, Qi F, et al. Incidence and risk factors of inguinal hernia occurred after radical prostatectomy-comparisons of different approaches. BMC Surg. 2020;20(1):218.
Nilsson H, Stranne J, Hugosson J, et al. Risk of hernia formation after radical prostatectomy: a comparison between open and robot-assisted laparoscopic radical prostatectomy within the prospectively controlled LAPPRO trial. Hernia. 2022;26:157–64.
Article CAS PubMed Google Scholar
Sim KC, Sung DJ, Han NY, et al. Preoperative CT findings of subclinical hernia can predict for postoperative inguinal hernia following robot-assisted laparoscopic radical prostatectomy. Abdom Radiol (NY). 2018;43:1231–6.
Otaki T, Hasegawa M, Yuzuriha S, et al. Clinical impact of psoas muscle volume on the development of inguinal hernia after robot-assisted radical prostatectomy. Surg Endosc. 2021;35:3320–8.
Alder R, Alder R, Rosenberg J. Incidence of Inguinal Hernia after Radical Prostatectomy: a systematic review and Meta-analysis. J Urol. 2020;203(2):265–74.
Lodding P, Bergdahl C, Nyberg M, et al. Inguinal hernia after radical retropubic prostatectomy for prostate cancer: a study of incidence and risk factors in comparison to no operation and lymphadenectomy. J Urol. 2001;166:964–7.
Sun M, Lughezzani G, Alasker A, et al. Comparative study of inguinal hernia repair after radical prostatectomy, prostate biopsy, transurethral resection of the prostate or pelvic lymph node dissection. J Urol. 2010;183:970–5.
Shimbo M, Endo F, Matsushita K, et al. Risk factors and a Novel Prevention technique for Inguinal Hernia after Robot-assisted radical prostatectomy. Urol Int. 2017;98:54–60. Incidence.
Chang KD, Abdel Raheem A, Santok GDR, et al. Anatomical Retzius-space preservation is associated with lower incidence of postoperative inguinal hernia development after robot-assisted radical prostatectomy. Hernia. 2017;21:555–61.
Matsubara A, Yoneda T, Nakamoto T, et al. Inguinal hernia after radical perineal prostatectomy: comparison with the retropubic approach. Urology. 2007;70:1152–6.
Iwamoto H, Morizane S, Hikita K, et al. Postoperative inguinal hernia after robotic-assisted radical prostatectomy for prostate cancer: evaluation of risk factors and recommendation of a convenient prophylactic procedure. Cent Eur J Urol. 2019;72(4):418–24.
Google Scholar
Download references
Acknowledgements
Not applicable.
This work was supported by the following funding: the grant 2019GY23 from Huzhou Science and Technology Bureau Public welfare application research project of China.
Author information
Authors and affiliations.
Department of Urology, The First People’s Hospital of Huzhou, #158, Square Road, Huzhou, 313000, China
Department of Urology, Huzhou Key Laboratory of Precise Diagnosis and Treatment of Urinary Tumors, Huzhou, 313000, China
An-Ping Xiang
You can also search for this author in PubMed Google Scholar
Contributions
An-Ping Xiang designed the study and drafted and revised the manuscript, Yue-Fan Shen recorded the patients cases, Xu-Feng Shen participated in the follow-up. An-Ping Xiang and Si-Hai Shao analyzes the data and draw graphs.
Corresponding author
Correspondence to Si-Hai Shao .
Ethics declarations
Ethics approval and consent to participate.
The study protocol was approved by the ethics committee of the First People’s Hospital of Huzhou (approval number, 2018137). We have obtained written informed consent from all study participants. All of the procedures were performed in accordance with the Declaration of Helsinki and relevant policies in China.
Consent for publication
Competing interests.
The authors declare no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Xiang, AP., Shen, YF., Shen, XF. et al. Correlation between the incidence of inguinal hernia and risk factors after radical prostatic cancer surgery: a case control study. BMC Urol 24 , 131 (2024). https://doi.org/10.1186/s12894-024-01493-w
Download citation
Received : 24 September 2023
Accepted : 30 April 2024
Published : 22 June 2024
DOI : https://doi.org/10.1186/s12894-024-01493-w
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
Search More Search for this keyword Advanced search
Latest content
For authors
Browse by collection
BMJ Journals
You are here
Volume 14, Issue 6
Photobiomodulation therapy for chronic knee pain in obese patients in pre-rehabilitation for bariatric surgery: randomised, placebo-controlled, double-blinded, clinical trial protocol
1 Biophotonics-Medicine Postgraduate Program , Universidade Nove de Julho , Sao Paulo , Brazil
2 Universidade Federal de Goias , Goiania , GO , Brazil
3 School of Medicine / Rehabilitation Rede Lucy Montoro / Unidade Morumbi , Universidade de São Paulo , Sao Paulo , Brazil
Correspondence to Professor Rebeca Boltes Cecatto; rebeca.boltes{at}gmail.com
Introduction Obesity has become a worldwide public health problem and is directly linked to loss of quality of life, complications and comorbidities. One of them is chronic pain, especially in the knees, which increases significantly and proportionally with weight gain. In patients with severe obesity, with indication for bariatric surgery, the presence of chronic pain disables and often prevents their participation in a pre-surgical rehabilitation programme. As an analgesic therapy, photobiomodulation (PBM) has been studied with safety, efficacy, well-tolerated used and low costs. Thus, this study aims to evaluate the use of PBM for the treatment of chronic knee pain in obese patients undergoing a pre-surgical rehabilitation programme for bariatric surgery.
Methods and analyses This is a double-blinded, randomised, placebo-controlled clinical, superiority, trial protocol. The PBM will be applied in bilateral knees and lumbar paraspinal points levels referring to the roots of innervation of the knee. The outcomes evaluated will be pain intensity, functionality, quality of life and clinical signs of neurological sensitization of chronic knee pain pathways.
Ethics and dissemination This protocol has already been approved by the Comitê de Ética em Pesquisa do Hospital das Clínicas da Universidade Federal de Goiás/EBSERH—Ethics Committee and it is following SPIRIT guidelines. The results will be statistically analysed and subsequently published in peer-reviewed journals.
Trial registration number Clinical Trials Platform ( https://clinicaltrials.gov/ ) with the number NCT05816798 .
Randomized Controlled Trial
REHABILITATION MEDICINE
Bariatric Surgery
Chronic Pain
COMPLEMENTARY MEDICINE
Physical Therapy Modalities
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/ .
https://doi.org/10.1136/bmjopen-2023-079864
Statistics from Altmetric.com
Request permissions.
If you wish to reuse any or all of this article please use the link below which will take you to the Copyright Clearance Center’s RightsLink service. You will be able to get a quick price and instant permission to reuse the content in many different ways.
STRENGTHS AND LIMITATIONS OF THIS STUDY
This protocol is a randomised, placebo, double-blinded controlled trial on photobiomodulation (PBM) treatment for obesity patients suffering from chronic pain.
The PBM protocol will be applied directly in the topography of pain associated with paraspinal stimulation targeting the origin of neural sensitization mechanisms of chronic pain.
Protocols aimed to apply to patients with chronic knee pain who have other comorbidities should be adapted to the particularities of these patients.
Since our sample will be composed of patients with pain with a minimum visual analogue scale of 40, we will include patients with pain ranging from moderate to high grade, which may impact the results, as patients with mild pain may not respond sufficiently to generate a statistical difference between the pre- and post-treatment moments.
Introduction
The world health panorama has shown a growing concern and allocation of resources to chronic diseases since these are the main reasons for increased disabilities and loss of quality of life worldwide. 1 2 Among these chronic conditions, obesity stands out. The WHO has recognised that obesity has become a public health concern. The Global Burden of Disease Study results showed that high body mass index (BMI) has become a major challenge, as it is directly linked to many health problems, such as cardiovascular, diabetes, kidney and neoplasm diseases. 2 3 In addition, chronic pain affects 33% of obese people and is also more prevalent in obese than non-obese patients. 4
Chronic musculoskeletal pain compromises the performance of daily and practical activities of obese individuals. Furthermore, longitudinal evidence shows that high BMI not only precedes but is also a predictor of knee pain. 5 Underweight individuals (BMI <18.5) had a prevalence of knee pain of 12.1%, those with desirable weight (BMI 18.5 and 24.9) had a prevalence of knee pain of 15.2%, and those with BMI ≧40 had a prevalence of knee pain of 55.7%. 6
In populations with severe obesity, bariatric surgery is indicated to reduce the risk of complications and comorbidities that arise due to excess weight. 7 Nonetheless, for a satisfactory result of bariatric surgery, it is necessary to carry out a pre-surgical rehabilitation programme consisting of therapeutic exercises aimed to improve cardiorespiratory fitness and mobility. 7 However, despite advances in therapeutic techniques aimed for analgesia, due to the chronicity and severity of pain, few advances are made functionally in these pre-surgical programmes, which impact negatively on clinical and functional post-surgical results. 8 The persistence of chronic knee pain in this population becomes a limitation for the individual’s daily activities, in addition to hindering their participation and adherence to the pre-rehabilitation programme for bariatric surgery. 5
Chronic pain does not only refer to pain that persists lasting longer than 3 months but is already well established to be related to central and peripheral neurological sensitization mechanisms with chronic pain, low response to conventional treatments, functional impact and poor prognosis. 9 In chronic pain therapy, the multimodal approach is more effective to control the symptoms. Medications that act on different anatomical sites of the pain pathway are needed. 9
In addition, non-pharmacological measures are also applied in a broad way. The use of cognitive-behavioural measures, exercises, proper nutrition, ergonomic modifications and physical therapies such as electric stimulation or photobiomodulation (PBM) is now considered a fundamental key point in the treatment of chronic pain. 10
PBM is an effective analgesic non-pharmacological therapy, which can be safely and easily applied by a qualified professional. The association of PBM with kinesiotherapy sessions may be a good option to alleviate pain and promote a faster return to functional status. 11–14 PBM refers to a series of therapies, in which non-ionising, non-thermal light beams, including LEDs and lasers in the visible and infrared spectra, are used for the interaction with biological tissues from different objectives. 15 Several possible mechanisms of action have been attributed to PBM such as an increase in endogenous opioids, thermal pain threshold, and local blood circulation, ATP or neurotransmitter production at the cellular level, and oxygen consumption and anti-inflammatory cytokine changes. 15
In this sense, numerous PBM techniques have been used in the treatment of musculoskeletal pain, and clinical studies have investigated its effectiveness with excellent results. 16 Thus, this study aimed to evaluate the effects of PBM on the pain and functionality of obese patients with chronic knee pain undergoing a pre-surgical rehabilitation programme for bariatric surgery, discussing its role as an analgesic therapy and modifier of neurological sensitization mechanisms to the pain pathway.
Methods and analyses
Study design, protocol registration and recruitment.
This will be a single-centre, superiority, phase II, double-blinded, randomised, two-arm, placebo-controlled clinical trial that will involve obese patients with a referral to bariatric surgery under medical follow-up in the Gastric Surgery Service of the Hospital das Clínicas da Universidade Federal de Goiás (HC-UFG) Brazil). It was registered in the Clinical Trials Platform ( https://clinicaltrials.gov/ ) with the number NCT05816798 and follows SPIRIT reporting guidelines. 17 To achieve adequate participant enrolment to reach the target sample size, participation in the study will be offered to all obese patients in the registry database of the medical group of the hospital with referral to bariatric surgery (BMI of over 40 or over 35 plus systemic disable conditions: sleep apnea, diabetes mellitus, coronary artery disease, arterial hypertension, dyslipidemia). Once identified in the database, the potentially eligible patients for the study will be contacted by the physiotherapists, who will explain the study and verify the interest in participating. If there is interest, evaluations will be made by the principal investigator (PI) to verify the eligibility criteria. Patient enrolment for this pilot study commenced in July 2023. To date, eight patients have been enrolled, with the anticipated pilot study enrolment completed by December 2024.
Eligibility criteria
An initial assessment will be conducted by the PI to assess the eligibility criteria and the signature of the consent form by the included patients.
Inclusion Criteria: Obese patients with chronic knee pain undergoing medical follow-up in the Gastric Surgery Service with an indication for bariatric surgery already performed by the responsible medical team and also submitted to the programme of pre-surgical rehabilitation standard treatment for bariatric surgery at the Physiotherapy Outpatient Clinic of the Hospital. These patients have already received the medical indication of the need to undergo surgery. However, even if the indication for the procedure is already established, as usual in the hospital routine, surgery is not performed immediately. They are submitted to a standard multidisciplinary pre-surgical rehabilitation programme preoperatively.
Patients with chronic pain (>3 months) in the knees bilaterally.
Based on studies by Üstün et al 18 and Matsuse et al 19 , we include obese patients with baseline knee pain assessed by the pain visual analogue scale (VAS) at least 40 at the moment of evaluation, using a 100 mm VAS with 0 representing no pain and 100 representing the worst pain imaginable.
Age: 18 to 70 years.
Agree to sign the Informed Consent Form approved by the local Ethics Committee.
Exclusion Criteria
Patients with a diagnosis of rheumatological, systemic inflammatory, knees previous musculoskeletal diseases, neuropathies, infections or tumours at the application site of therapy, severe psychiatric disorders requiring psychiatric care.
Previous use of phototherapy for the same or another indication.
Use of corticosteroids at an immunosuppressive dose (20 mg daily of prednisone or equivalent for at least 14 days) in the last 90 days.
Systemic injections and/or joint infiltrations of corticoids or hyaluronic acid in the last 3 months.
Withdrawal of the Informed Consent form by the participant.
Patients excluded from the queue for bariatric surgery or the pre-surgical rehabilitation programme.
Changes in the analgesic medication used. Changes in the dosages may be tolerated as long as there are no changes in the class of medication. The dosage modifications throughout the study, if they occur, will be described.
Randomisation and allocation
Eligible patients will be assigned to groups with a 1:1 allocation rate into two groups. The two groups are the PBM intervention group (use of PBM therapy+pre-surgical rehabilitation standard programme of the hospital) or control group (placebo PBM therapy+pre-surgical rehabilitation standard programme of the hospital). At the time of allocation, opaque envelopes will be identified with sequential numbers with the information on the corresponding group according to the order obtained in the randomisation list by Research Randomiser online software, which generates a sequential randomisation list using random block sizes (eight patients per block). The envelopes will be sealed in numerical order until the moment of study intervention and just immediately before the PBM moment, the researcher responsible for the treatment will open one envelope (without changing the numerical sequence) and perform the indicated procedure (PBM or placebo PBM).
Baseline and final assessments will be conducted by the PI, who will be blinded about the randomisation and allocation of patients. Patients will also be blinded to the randomisation and allocation until the end of the study. The pre-surgical rehabilitation standard treatment will be held by a physiotherapist who is blinded to evaluation data or the treatment group. Another physiotherapist will be responsible for the application of PBM, placebo PBM and by the allocation and randomisation, but is also blinded to evaluation data. Concerning placebo treatment, our participants do not use PBM therapy routinely, and they are not familiar with the procedures or particularities of this therapy, which contributes to their inability to distinguish between regular therapy and placebo therapy. Furthermore, all participants will wear dark protective glasses, which completely block vision (used for eye safety) and contribute to the blinding of using a placebo. The recorded sound that will be used to simulate the use of the equipment (placebo PBM group) is the sound generated by the device itself in use, during its regular operation in the study.
Sample size
The sample size was calculated based on Matsuse et al 19 in which VAS values were obtained for the control group (61.5±22.8) and the treated group (44.2±19.4), with a reliability of 95%, error of 5% and test detection power of 80%. Considering a VAS change of at least 20% comparing the pre and post-moments in the treatment group, the minimum sample size will be 26 patients per group. Assuming a percentage of 20% of drop-outs, the minimum sample size will be 31 patients per group. 19
Interventions
1. Pre-surgical rehabilitation standard programme of the hospital
All patients undergoing follow-up at the Gastric Outpatient Clinic of HC-UFG due to severe obesity and who have an indication for bariatric surgery are submitted to a standard multidisciplinary pre-surgical rehabilitation programme for 3 to 6 months preoperatively.
This programme will be maintained for all study patients, for both groups, throughout the study period and includes 2X per week activities of:
Cardiopulmonary physiotherapy: depending on the clinical condition may include deep breathing exercises; hands-on techniques; breathing facilitation exercises; percussions and vibrations; coughing and breathing strategies; circulation exercises; mobility assistance to move safely in bed; and sit up, stand, walk, bed and chair standing exercises to prevent deep vein thrombosis (clots) using the fitness programme.
Kinesiotherapy with global muscle strengthening exercises: depending on the clinical condition, these may include lifting weights, working with resistance bands, climbing stairs, hill walking, cycling, dance, push-ups, sit-ups and squats.
Follow-up with the nutrition team to personalised, one-on-one dietary guidance and counselling.
Follow-up with the psychology team to personalised one-on-one identify barriers, come up with strategies, solve problems and assist the patients in figuring out how they are going to implement some of the needed changes given their individual life circumstance.
2. PBM intervention Group
In addition to the standard treatment described above, the PBM therapy sessions will be carried out in the Physiotherapy Outpatient Clinic of the Hospital, two times per week, for 12 consecutive weeks, just after the pre-surgical rehabilitation standard programme, to improve adherence to intervention protocols. The PBM application points are as follows:
Transcutaneous paravertebral region bilaterally at levels of L3, L4 (iliac crest), L5, S1 and, S2 roots topography, 1 cm lateral to the spinous process, corresponding to the roots levels that innervate the knee joint (totaling 10 paraspinal points).
Knees transcutaneous bilaterally (four points on each knee):
Anteromedial point.
Anterolateral point.
Patellofemoral joint—the apex of the patella.
Patellofemoral-base patellar joint.
The responsible for the application will be present throughout the intervention.
The PBM parameters are described in table 1 and are based on studies by Fernandes et al , Zein et al , and Leal-Junior et al . 11 20 21 They also follow the recommendations of the World Association of Laser Therapy WALT. 20–22
View inline
Photobiomodulation parameters
3. Placebo PBM therapy
Placebo group patients will receive the pre-surgical rehabilitation standard programme described above as well as a placebo PBM treatment to mask the treatment. The placebo PBM therapy has the same procedures, number of points and place of application described in the item PBM intervention group; however, the PBM equipment will be turned off. The device activation noise will be recorded and used to mimic the irradiation.
Furthermore, the PBM therapy and placebo PBM therapy will be performed on the same day that the patient is already scheduled to undergo the pre-surgical rehabilitation standard programme of the hospital, therefore not adding extra-hospital visits for the patients.
Outcomes and measures
The primary outcomes evaluated will be pain and functionality through the following outcome measures:
Change from baseline to 12 weeks (after PBM treatment) in the VAS. 23 24 Pain knee was evaluated using a 100 mm VAS with 0 representing no pain and 100 representing the worst pain imaginable.
Change from baseline to 12 weeks (after PBM treatment) in the Brazilian version of Knee Injury and Osteoarthritis Outcome Score Questionnaire 25 .
Secondary outcomes related to the clinical assessment of neurological sensitization of the pain pathway will be evaluated through:
Changes from baseline to 12 weeks (after PBM treatment) in the pressure pain threshold measured bilaterally in the muscles: popliteus, sartorius, quadratus lumborum, rectus femoris, vastus medialis, vastus lateralis, adductor longus, tibialis anterior, peroneus longus, gracilis and supraspinatus ligaments between L1-L2, L2-L3, L3-L4, L4-L5, L5-S1 and S1-S2. 26 27 Pressure is applied perpendicularly to the skin at a speed of 1 kg/s by a digital pressure algometer (Instrutherm TM ) to patients indicate when they start to feel pain.
Changes from baseline to 12 weeks (after PBM treatment) in the the Pinch and Roll Maneauver 26 28 29 at L1, L2, L3, L4, L5, S1 and S2 will be performed bilaterally to assess signs of subcutaneous hyperalgesia.
Other exploratory outcomes are related to knee function and quality of life through the following outcome measures:
Changes from baseline to 12 weeks (after PBM treatment) in the 6 min walk test. 30
Changes from baseline to 12 weeks (after PBM treatment) in the Brazilian version of the SF 36 Quality of Life Scale. 31
Changes from baseline to 12 weeks (after PBM treatment) in the range of motion of the knee joint measured with a goniometer.
The following data will be collected from medical official records for the sample epidemiological clinical data: age, gender, BMI, life habits (alcoholism, smoking, drug use), comorbidities, use of analgesic drugs and doses and knee pain duration.
The schedule of enrolment, interventions, assessments and visits for participants is presented in figure 1 . Figure 2 presents the planned flow chart showing inclusion, randomisation and participation throughout the study.
Download figure
Open in new tab
Download powerpoint
Participant timeline schedule of enrolment, interventions and assessments.
The planned flow chart showing inclusion, randomisation and participation throughout the study.
Data collection and monitoring
An electronic spreadsheet database will be created to preserve the confidentiality of patient data and allow the exchange of information between the researchers of the group. This information will be stored for 5 years after the completion of the study in a digital file by the PI. All research data collected will be saved directly in these electronic files and stored on the research team’s institutional drive server. The system has authentication password tools, access control and activity recording, ensuring security and traceability of data.
Statistical analyses
The data will be analysed to assess the distribution of demographic data and outcome criteria by the Kolmgorov–Smirnov (KS) and Shapiro–Wilk tests. Variables are reported as means and SD. Comparison of before/after PBM ‘within group’ will be made using paired t-test. Comparison of changes from baseline to the endpoint (treatment vs sham) ‘between groups’, will be made with two-sample t-test. In case of non-normal distribution, comparisons will be made using the Wilcoxon Sign Rank test and Mann–Whitney test for paired and unpaired data, respectively. To analyse the correlation of primary and secondary outcomes the χ2 test or Pearson’s exact test will be used. For all tests, a significance level of α=5% will be established. All analyses will be performed using SPSS statistical software version 28.0 for MAC (IBM Corporation, USA).
Patient and public involvement
Patients or the public were not involved in the design, conduct, reporting or dissemination plans of our research.
ETHICS AND DISSEMINATION PLAN
This study complies with the ethical research guidelines already approved by the ethics committee of the Comitê de Ética em Pesquisa do Hospital das Clínicas da Universidade Federal de Goiás/EBSERH-Ethics Committee with the number 5.951.619/approval number: 66250922200005078. The participants will only be included after properly obtaining consent and signing the Free and Informed Consent term. All data published or made available will not contain sensitive data that identify the patients. The study will not interfere with the clinical follow-up and medical decisions of the healthcare team or medical routine of patients.
Safety/harms
Although the use of PBM devices is safe, the main care should be directed towards avoiding ocular injury (damage to the retina, lens such as cataracts, burns to the cornea and crystalline lens) and skin damage, such as burns, erythema and increased sensitivity. 32 To prevent these side effects, during the interventions, both examiners and patients will be wearing protective eyewear. Moreover, applications will occur after locally cleaning the device and skin. In addition, our clinical team of study has experiences and qualifications in the application of PBM therapies. After each therapeutic session, the patient will be questioned and clinically evaluated for any undesirable or adverse effect of the PBM (Adverse Effects Monitoring Sheet) by the health professional team. If there is any Suspected Unexpected Serious Adverse Reaction, the patient will be removed from the study, and the Ethical Committee will be notified to assess the need to interrupt the intervention/study and/or unblinding patients. If any other medical treatment is necessary, it will be carried out by the hospital medical team. If any adverse event occurs, participants will be withdrawn from the study, and these data will be reported. Any withdrawal or loss of patients due to adverse events will be reported.
Dissemination Plan
The data management plan is available in the Data Management Plan https://dmphub.uc3prd.cdlib.net/dmps/10.48321/D1MW8J
Upon completion of the study, the original clinical non-identifiable collected data stored in the spreadsheets of institutional drive referring to pain, quality of life and functionality assessments will be made available in an open science repository, to collaborate with the scientific community and auditing. The results of this work after the statistical analysis (whether they are favorable or not) will be published in a peer-reviewed scientific journals.
Ethics statements
Patient consent for publication.
Not applicable.
Ethics approval
This study complies with the ethical research guidelines, already approved by the ethics committee by the Comitê de Ética em Pesquisa do Hospital das Clínicas da Universidade Federal de Goiás/EBSERH-Ethics Committee with the number 5.951.619 / Approval Number: 66250922200005078.
Acknowledgments
We acknowledge and appreciate the statistical support by José Eduardo Corrente/ Sigma Scientific consulting, Botucatu - SP.
Arora M , et al
Alsalhe TA ,
Chalghaf N , et al
Huang W-L ,
Akter S , et al
Zdziarski LA ,
Wasser JG ,
Andersen RE ,
Crespo CJ ,
Bartlett SJ , et al
Arterburn DE ,
Kushner RF , et al
Peltonen M ,
Lindroos AK ,
Torgerson JS
Martin LF ,
Slepian MJ , et al
Leal-Junior ECP ,
Johnson DS ,
Saltmarche A , et al
A Hamid MS ,
Dutta N , et al
Stausholm MB ,
Naterstad IF ,
Joensen J , et al
Moncrieff L ,
Matys J , et al
Clijsen R ,
Brunner A ,
Barbero M , et al
Tetzlaff JM ,
Altman DG , et al
Gülçiçek OB , et al
Matsuse H ,
Rabe KG , et al
Fernandes K ,
Ferrari R ,
Selting W ,
↵ WALT Recommended treatment doses for low level laser therapy 780-860 nm wavelength: world association for laser therapy , 2010 . Available : https://waltpbm.org/wp-content/uploads/2021/08/Dose_table_780-860nm_for_Low_Level_Laser_Therapy_WALT-2010.pdf
Jensen MP ,
Hawker GA ,
Kendzerska T , et al
Almeida GPL
Imamura M ,
Imamura ST ,
Kaziyama HHS , et al
Ezquerro F ,
Marcon Alfieri F , et al
Simonsen O , et al
Farasyn AD ,
Meeusen R ,
Andrade GN ,
Shima P , et al
Ciconelli RM
Hamblin M ,
Contributors Author Contributions: conceptualisation, ACFGA, RBC, TCFB, TNSD and FARJ; study design/methodology, ACFGA and RBC; writing original draft preparation, ACFGA and RBC; writing—review and editing, RLM, ALSF, MFSDR, ACFGA, TCFB, TNSD, FARJ, RLM, ALSF, MFSDR and RBC; supervision, RBC; and project administration, ACFGA and RBC.
Funding This study was supported by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES) through Universidade Nove de Julho / UNINOVE / Brazil, Programa de Excelência Acadêmica PROEX, 88887.818181/2023-00.
Competing interests The authors declare no competing interests
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Read the full text or download the PDF:
Clinical analysis of 23 cases of epidermoid cyst of testis in children
Original Article
Published: 02 July 2024
Volume 40 , article number 165 , ( 2024 )
Cite this article
Jie Tao 1 , 2 , 3 ,
Fei Chen 1 , 2 , 3 ,
Xia Chen 1 , 2 , 3 &
Junhong Liu 1 , 2 , 3
This study aims to examine the clinical characteristics and surgical management of pediatric testicular epidermoid cysts, thereby contributing to the existing body of knowledge pertinent to the diagnosis and therapeutic intervention 你 s for this condition.
A retrospective analysis was conducted on the clinical records of 23 pediatric patients diagnosed with testicular epidermoid cysts, who were admitted to our institution between April 2013 and February 2024. Concurrently, a comprehensive review and analysis of pertinent literature were undertaken to augment the findings.
The mean age at which the onset of epidermoid cysts was observed was 6.0 years. All cases were singular and unilateral. B-ultrasound diagnosis categorized 6 cases as epidermoid cysts, 11 as teratomas, and 6 as indeterminate, yielding a diagnostic sensitivity of 26.1%. All patients underwent testicle-sparing mass resection, and nine patients underwent rapid intraoperative frozen section analysis, revealing eight cases of testicular epidermoid cysts and one teratoma, with a diagnostic sensitivity of 88.89%. Postoperative histopathological examination confirmed the diagnosis of testicular epidermoid cyst.
Conclusions
Pediatric testicular epidermoid cysts are an uncommon occurrence, primarily presenting as a painless scrotal mass, which can mimic the clinical features of malignant testicular tumors. Imaging modalities and histopathological assessment are pivotal in the diagnostic process for pediatric testicular epidermoid cysts. For cases where B-ultrasound is inconclusive, rapid intraoperative pathological examination should be considered.
This is a preview of subscription content, log in via an institution to check access.
Access this article
Subscribe and save.
Get 10 units per month
Download Article/Chapter or Ebook
1 Unit = 1 Article or 1 Chapter
Cancel anytime
Price includes VAT (Russian Federation)
Instant access to the full article PDF.
Rent this article via DeepDyve
Institutional subscriptions
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Shah KH, Maxted WC, Chun B (1981) Epidermoid cysts of the testis: a report of three cases and an analysis of 141 cases from the world literature. Cancer 47(3):577–582
Article CAS PubMed Google Scholar
Loya AG, Said JW, Grant EG (2004) Epidermoid cyst of the testis: radiologic-pathologic correlation. Radiographics 24(Suppl 1):S243–S246
Article PubMed Google Scholar
Liu Y, Pan Y, Wang Z (2022) MRI diagnostic value of epidermoid cyst of testis. J Med Imaging 32(11):2025–2029
Google Scholar
Arellano CM et al (2011) Testicular epidermoid cysts in children: sonographic characteristics with pathological correlation. Pediatr Radiol 41(6):683–689
Maulana R, Siregar S, Hernowo BS (2022) Testicular epidermoid cyst: a rare case report. Int J Surg Case Rep 94:107167
Article PubMed PubMed Central Google Scholar
Dogra VS et al (2001) Testicular epidermoid cysts: sonographic features with histopathologic correlation. J Clin Ultrasound 29(3):192–196
Li Y et al (2022) Research progress of epidermoid cyst of testis. Cancer Prog 20(07):656–658
Win ML et al (2020) Bilateral testicular epidermoid cysts in a man with klinefelter syndrome: a case report. Cureus 12(12):e11834
PubMed PubMed Central Google Scholar
Zhang J, Li Y (2022) Value of high frequency ultrasonography in diagnosing epidermoid cyst of testis. J Shandong Med College 44(04):309–310
Rong H, Gao N, Wang D (2022) The value of high frequency ultrasound combined with alpha-fetoprotein detection in the accurate and qualitative diagnosis of testicular tumors in children. Basic Clin Oncol 35(06):525–527
Price EJ (1969) Epidermoid cysts of the testis: a clinical and pathologic analysis of 69 cases from the testicular tumor registry. J Urol 102(6):708–713
Changli Xu et al (2019) Epidermoid cyst of testis: report of 5 cases and literature review. Chin J Androl 33(05):60–62
Download references
Acknowledgements
The authors would like to thank the parents and children who enrolled in the study and the health professionals from the department of ultrasonography. Their outstanding support and contributions are gratefully appreciated.
No funding.
Author information
Authors and affiliations.
Department of Day Surgery, National Clinical Research Center for Child Health and Disorders, Ministry of Education, Key Laboratory of Child Development and Disorder, Children’s Hospital of Chongqing Medical University, Chongqing, China
Jie Tao, Fei Chen, Xia Chen & Junhong Liu
China International Science and Technology Cooperation Base of Child Development and Critical Disorders, Chongqing, China
Chongqing Key Laboratory of Structural Birth Defect and Reconstruction, Chongqing, China
You can also search for this author in PubMed Google Scholar
Contributions
All authors have worked on the manuscript. Jie Tao wrote the manuscript under the supervision of Junhong Liu. Fei Chen and Xia Chen followed up the patient.
Corresponding author
Correspondence to Junhong Liu .
Ethics declarations
Conflict of interest.
The authors declare that they have no conflict of interest.
Ethical approval
This retrospective study involving human participants was in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Additional information
Publisher's note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
Reprints and permissions
About this article
Tao, J., Chen, F., Chen, X. et al. Clinical analysis of 23 cases of epidermoid cyst of testis in children. Pediatr Surg Int 40 , 165 (2024). https://doi.org/10.1007/s00383-024-05750-9
Download citation
Accepted : 24 June 2024
Published : 02 July 2024
DOI : https://doi.org/10.1007/s00383-024-05750-9
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
Wrong-site surgery occurs in all surgical specialties but is most common among ... one study showed that preoperative signing of ... healing for the patient. In this case, despite Dr. Ring's ...
Case 24-2020: A 44-Year-Old Woman with Chest Pain, Dyspnea, and Shock
A 44-year-old woman presented with cough, dyspnea, and chest pain. On examination, she had tachycardia and hypotension. Evaluation revealed SARS-CoV-2 RNA in a nasopharyngeal swab, as well as eleva...
Case 22-2020: A 62-Year-Old Woman with Early Breast Cancer during the
In one study, 69.8% of the patients had a partial or ... allowing the patient to make a more informed surgical decision regarding breast-conserving therapy or mastectomy. ... et al. Case fatality ...
PDF BEST PRACTICES CASE STUDIES
The 2020 Best Practices Case Studies were selected from a bank of more than 450 abstracts submitted for the 2020 ACS Quality and Safety Conference. All abstracts were reviewed and vetted by a panel of program experts, and the authors of the studies chosen were asked to further develop their case study and share their accomplishments.
ACS Case Reviews in Surgery
ACS Case Reviews in Surgery is a unique, peer-reviewed, open access, online-only case report journal published six times a year that presents high-quality, in-depth analyses of actual surgical cases. The journal boasts an exceptional editorial and reviewer board comprised of distinguished surgeon leaders from around the world.
Case Studies
Case Studies. In this section we report a variety of clinical cases in an effort to share our experience with healthcare providers and with patients who may benefit. The cases are categorized into a wide variety of different medical and surgical specialties listed under subheadings. The main objective is to share our knowledge and experience ...
Care of the surgical patient: part 1
This article provides clinical guidance on the care of a patient undergoing an elective surgical procedure. It discusses preoperative care and the preparation of the patient. It aims to provide an awareness of the complications associated with perioperative care. Through the use of a patient case study, the authors demonstrate the care required ...
Case Study: Cardiac Surgery
Dr. John Conte performed the coronary bypass surgery. Of interest is the fact that in 1999, Dr. Conte published a case report of the first ever successful bloodless lung transplant in a Jehovah's Witness patient. In this case presented here, he decided the patient would be best served by performing an "off-pump" cardiac surgery where the ...
Case Study: Vascular Surgery
Case Study 1: Revision Surgery for Thoracic and Abdominal Aortic Aneurysm Using a Minimally Invasive Endovascular Fenestrated Stent Graft. An 81-year old female patient (Jehovah's Witness) presented with an expanding aortic aneurysm in the thoraco-abdominal (chest and abdomen) region that had enlarged from 5 to 7 centimeters.
Care of the surgical patient: part 1
Abstract. This article provides clinical guidance on the care of a patient undergoing an elective surgical procedure. It discusses preoperative care and the preparation of the patient. It aims to provide an awareness of the complications associated with perioperative care. Through the use of a patient case study, the authors demonstrate the ...
Case Study: Repair Surgery for Patient with Hernia and Abdominal Damage
Treating a patient after a complicated hernia repair led to surgical complications and chronic pain. A 55-year-old woman with a history of Crohn's disease presented after having multiple hernia surgeries. The patient explained that in 2018, she saw a surgeon at an outside hospital who offered her a robotic-assisted abdominal wall reconstruction.
Case Study: Surgical Reconstruction in a Single Patient with Bilateral
In the case study, Surgical Reconstruction in a Single Patient with Bilateral Avascular Necrosis of the Talus, first author Kanika Kochhar, DPM, along with co-authors Cara Fontana, DPM and Brandon Gumbiner, DPM, highlight the outcomes of a female patient with severe foot and ankle deformity secondary to CN and avascular necrosis (AVN) of the ...
The Surgical Patient on Critical Care (Chapter 38)
Chapter 38 - The Surgical Patient on Critical Care. Published online by Cambridge University Press: 04 May 2017. By. John Jameson. Edited by. Daniele Bryden and. Andrew Temple. Chapter. Get access.
Faculty Case Studies
The case studies are contained in 4 categories: Family (13 case studies), Fundamentals and Mental Health (14 case studies) and Medical Surgical (20 case studies). In addition the folder labeled minireviews contains PowerPoint sessions with combinations of case studies and standalone items.
Case Study
The results for improving the laminectomy surgical setup were very impressive. After implementing the build-to-order sets, the instrument assembly went from 34 minutes to 20 minutes, 15 seconds. The instrument setup in the OR went from 24 minutes, 9 seconds, to 2 minutes, 29 seconds — a 90 percent decrease.
Course Case Studies
CASE STUDY 1. Patient A is a man 37 years of age who arrives in the PACU following surgical removal of his gallbladder. Surgical intervention using the laparoscopic approach is successful. Patient A's airway and ability to maintain respiratory stability are evaluated immediately.
Risk Factors for Postoperative Pneumonia: A Case-Control Study
A matched 1:1 case-control study, including adult patients who underwent surgery between January 2020 and June 2020, was conducted in the Second Affiliated Hospital of Kunming Medical University in China. ... A total of 17,190 surgical patients were selected for the study, of which 264 patients were diagnosed with postoperative pneumonia ...
Articles
Here we report a case of De Garengeot's hernia that occurred in a male patient who had a history of inguinal hernia surgery ... Shiro Fujihata, Hiromasa Kuzuya, Masaaki Kurimoto, Tadashi Shibata, Hirozumi Sawai and Shuji Takiguchi. Surgical Case Reports 2024 10 :132. Case Report Published on: 29 May 2024.
Preoperative Evaluation of the Surgical Patient
Preoperative evaluation is a process of clinical assessment that precedes the delivery of anesthesia care for surgery and non-surgical procedures. At the very least, it includes a review of medical records and recent test results, a comprehensive medical history, and a physical examination of the cardiovascular system, the pulmonary system, and ...
How to present patient cases
Presenting patient cases is a key part of everyday clinical practice. A well delivered presentation has the potential to facilitate patient care and improve efficiency on ward rounds, as well as a means of teaching and assessing clinical competence. 1 The purpose of a case presentation is to communicate your diagnostic reasoning to the listener, so that he or she has a clear picture of the ...
Surgical Case Reports
Scope of Journal. Surgical Case Reports (SCR) is a dedicated platform aiming to advance the understanding and practice of surgery. Our principal goal is to provide a global forum where clinicians, surgeons, and researchers can share, learn, and discuss novel surgical techniques, treatments, and patient case studies that contribute to the field's progress.
Patient Outcome Measures Within a Surgical Quality Improvement Program
Key Points. Question Is it feasible to leverage health information technology to collect patient-reported outcome measures (PROMs) within a national surgical quality improvement program at scale?. Findings This pragmatic cohort study of 65 hospitals (including 130 365 patients) participating in the American College of Surgeons National Surgical Quality Improvement Program achieved the 30% or ...
Case study/practice questions care of surgical patients
D.Insertion of a surgical drain. A.Diabetes mellitus. The risk for infection is higher in patients with pre-existing health problems such as diabetes mellitus, immune deficiency, obesity, and kidney failure. A surgical drain allows for removal of secretions and fluids from within the tissues around the surgical area.
Case Study: Surgical Oncology
Case Study: Surgical Oncology. ... There was no need for veno-veno bypass as the patient tolerated the partial cross clamp with hemodynamic stability. The blood loss was substantial (1,200 mLs) which for her body mass (50kg) was about 1/3 of her entire blood volume (calculated as 70 mL per kg or 3,500 mLs). The shed blood was processed through ...
Adverse postoperative outcomes in elderly patients with sarcopenia
Study cohort. The data of 60,790 surgical patients (i.e., 12,158 and 48,632 in the sarcopenia and nonsarcopenia groups, respectively) were included in this study for further analysis; their characteristics are listed in Table 1.After frequency matching, the between-group differences in age, sex, income levels, urbanization, coexisting medical conditions, hospital levels, types of anesthesia ...
Effect of individualized anesthesia and ...
Worldwide, there are more than 230 million surgical procedures performed every year and it is estimated that 20%-80% of patients undergoing these procedures will suffer acute postoperative pain (APOP). 1-3 Known surgical risk factors for APOP are large incisions and a type of procedure. 4, 5 Acute postoperative pain is associated with the ...
Correlation between the incidence of inguinal hernia and risk factors
The incidence of recurrent hernia after radical resection of prostate cancer is high, so this article discusses the incidence and risk factors of inguinal hernia after radical resection of prostate cancer. This case control study was conducted in The First People's Hospital of Huzhou clinical data of 251 cases underwent radical resection of prostate cancer in this hospital from March 2019 to ...
Photobiomodulation therapy for chronic knee pain in obese patients in
Thus, this study aims to evaluate the use of PBM for the treatment of chronic knee pain in obese patients undergoing a pre-surgical rehabilitation programme for bariatric surgery. Methods and analyses This is a double-blinded, randomised, placebo-controlled clinical, superiority, trial protocol.
Extracranial Head and Neck Schwannomas: A Single Centre ...
The study included 97 patients; of them, 52.6% were male, and 47.4% were female. The median age of study population was 36 years. ... nasal bleeding in 1 case, and loosening of teeth in 1 case. Ear-related complaints were present in 10.3% of the total patients. ... and one patient developed a surgical site infection that was managed ...
Clinical analysis of 23 cases of epidermoid cyst of testis ...
Objective This study aims to examine the clinical characteristics and surgical management of pediatric testicular epidermoid cysts, thereby contributing to the existing body of knowledge pertinent to the diagnosis and therapeutic intervention 你 s for this condition. Methods A retrospective analysis was conducted on the clinical records of 23 pediatric patients diagnosed with testicular ...








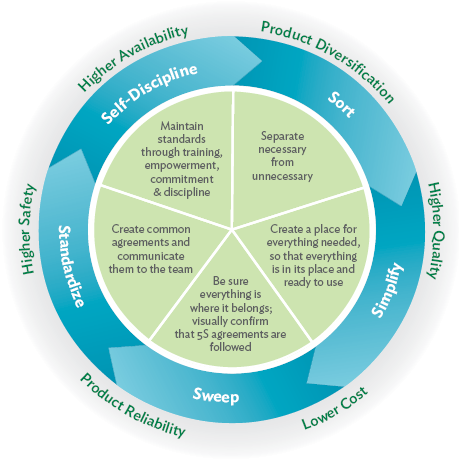















COMMENTS
Wrong-site surgery occurs in all surgical specialties but is most common among ... one study showed that preoperative signing of ... healing for the patient. In this case, despite Dr. Ring's ...
A 44-year-old woman presented with cough, dyspnea, and chest pain. On examination, she had tachycardia and hypotension. Evaluation revealed SARS-CoV-2 RNA in a nasopharyngeal swab, as well as eleva...
In one study, 69.8% of the patients had a partial or ... allowing the patient to make a more informed surgical decision regarding breast-conserving therapy or mastectomy. ... et al. Case fatality ...
The 2020 Best Practices Case Studies were selected from a bank of more than 450 abstracts submitted for the 2020 ACS Quality and Safety Conference. All abstracts were reviewed and vetted by a panel of program experts, and the authors of the studies chosen were asked to further develop their case study and share their accomplishments.
ACS Case Reviews in Surgery is a unique, peer-reviewed, open access, online-only case report journal published six times a year that presents high-quality, in-depth analyses of actual surgical cases. The journal boasts an exceptional editorial and reviewer board comprised of distinguished surgeon leaders from around the world.
Case Studies. In this section we report a variety of clinical cases in an effort to share our experience with healthcare providers and with patients who may benefit. The cases are categorized into a wide variety of different medical and surgical specialties listed under subheadings. The main objective is to share our knowledge and experience ...
This article provides clinical guidance on the care of a patient undergoing an elective surgical procedure. It discusses preoperative care and the preparation of the patient. It aims to provide an awareness of the complications associated with perioperative care. Through the use of a patient case study, the authors demonstrate the care required ...
Dr. John Conte performed the coronary bypass surgery. Of interest is the fact that in 1999, Dr. Conte published a case report of the first ever successful bloodless lung transplant in a Jehovah's Witness patient. In this case presented here, he decided the patient would be best served by performing an "off-pump" cardiac surgery where the ...
Case Study 1: Revision Surgery for Thoracic and Abdominal Aortic Aneurysm Using a Minimally Invasive Endovascular Fenestrated Stent Graft. An 81-year old female patient (Jehovah's Witness) presented with an expanding aortic aneurysm in the thoraco-abdominal (chest and abdomen) region that had enlarged from 5 to 7 centimeters.
Abstract. This article provides clinical guidance on the care of a patient undergoing an elective surgical procedure. It discusses preoperative care and the preparation of the patient. It aims to provide an awareness of the complications associated with perioperative care. Through the use of a patient case study, the authors demonstrate the ...
Treating a patient after a complicated hernia repair led to surgical complications and chronic pain. A 55-year-old woman with a history of Crohn's disease presented after having multiple hernia surgeries. The patient explained that in 2018, she saw a surgeon at an outside hospital who offered her a robotic-assisted abdominal wall reconstruction.
In the case study, Surgical Reconstruction in a Single Patient with Bilateral Avascular Necrosis of the Talus, first author Kanika Kochhar, DPM, along with co-authors Cara Fontana, DPM and Brandon Gumbiner, DPM, highlight the outcomes of a female patient with severe foot and ankle deformity secondary to CN and avascular necrosis (AVN) of the ...
Chapter 38 - The Surgical Patient on Critical Care. Published online by Cambridge University Press: 04 May 2017. By. John Jameson. Edited by. Daniele Bryden and. Andrew Temple. Chapter. Get access.
The case studies are contained in 4 categories: Family (13 case studies), Fundamentals and Mental Health (14 case studies) and Medical Surgical (20 case studies). In addition the folder labeled minireviews contains PowerPoint sessions with combinations of case studies and standalone items.
The results for improving the laminectomy surgical setup were very impressive. After implementing the build-to-order sets, the instrument assembly went from 34 minutes to 20 minutes, 15 seconds. The instrument setup in the OR went from 24 minutes, 9 seconds, to 2 minutes, 29 seconds — a 90 percent decrease.
CASE STUDY 1. Patient A is a man 37 years of age who arrives in the PACU following surgical removal of his gallbladder. Surgical intervention using the laparoscopic approach is successful. Patient A's airway and ability to maintain respiratory stability are evaluated immediately.
A matched 1:1 case-control study, including adult patients who underwent surgery between January 2020 and June 2020, was conducted in the Second Affiliated Hospital of Kunming Medical University in China. ... A total of 17,190 surgical patients were selected for the study, of which 264 patients were diagnosed with postoperative pneumonia ...
Here we report a case of De Garengeot's hernia that occurred in a male patient who had a history of inguinal hernia surgery ... Shiro Fujihata, Hiromasa Kuzuya, Masaaki Kurimoto, Tadashi Shibata, Hirozumi Sawai and Shuji Takiguchi. Surgical Case Reports 2024 10 :132. Case Report Published on: 29 May 2024.
Preoperative evaluation is a process of clinical assessment that precedes the delivery of anesthesia care for surgery and non-surgical procedures. At the very least, it includes a review of medical records and recent test results, a comprehensive medical history, and a physical examination of the cardiovascular system, the pulmonary system, and ...
Presenting patient cases is a key part of everyday clinical practice. A well delivered presentation has the potential to facilitate patient care and improve efficiency on ward rounds, as well as a means of teaching and assessing clinical competence. 1 The purpose of a case presentation is to communicate your diagnostic reasoning to the listener, so that he or she has a clear picture of the ...
Scope of Journal. Surgical Case Reports (SCR) is a dedicated platform aiming to advance the understanding and practice of surgery. Our principal goal is to provide a global forum where clinicians, surgeons, and researchers can share, learn, and discuss novel surgical techniques, treatments, and patient case studies that contribute to the field's progress.
Key Points. Question Is it feasible to leverage health information technology to collect patient-reported outcome measures (PROMs) within a national surgical quality improvement program at scale?. Findings This pragmatic cohort study of 65 hospitals (including 130 365 patients) participating in the American College of Surgeons National Surgical Quality Improvement Program achieved the 30% or ...
D.Insertion of a surgical drain. A.Diabetes mellitus. The risk for infection is higher in patients with pre-existing health problems such as diabetes mellitus, immune deficiency, obesity, and kidney failure. A surgical drain allows for removal of secretions and fluids from within the tissues around the surgical area.
Case Study: Surgical Oncology. ... There was no need for veno-veno bypass as the patient tolerated the partial cross clamp with hemodynamic stability. The blood loss was substantial (1,200 mLs) which for her body mass (50kg) was about 1/3 of her entire blood volume (calculated as 70 mL per kg or 3,500 mLs). The shed blood was processed through ...
Study cohort. The data of 60,790 surgical patients (i.e., 12,158 and 48,632 in the sarcopenia and nonsarcopenia groups, respectively) were included in this study for further analysis; their characteristics are listed in Table 1.After frequency matching, the between-group differences in age, sex, income levels, urbanization, coexisting medical conditions, hospital levels, types of anesthesia ...
Worldwide, there are more than 230 million surgical procedures performed every year and it is estimated that 20%-80% of patients undergoing these procedures will suffer acute postoperative pain (APOP). 1-3 Known surgical risk factors for APOP are large incisions and a type of procedure. 4, 5 Acute postoperative pain is associated with the ...
The incidence of recurrent hernia after radical resection of prostate cancer is high, so this article discusses the incidence and risk factors of inguinal hernia after radical resection of prostate cancer. This case control study was conducted in The First People's Hospital of Huzhou clinical data of 251 cases underwent radical resection of prostate cancer in this hospital from March 2019 to ...
Thus, this study aims to evaluate the use of PBM for the treatment of chronic knee pain in obese patients undergoing a pre-surgical rehabilitation programme for bariatric surgery. Methods and analyses This is a double-blinded, randomised, placebo-controlled clinical, superiority, trial protocol.
The study included 97 patients; of them, 52.6% were male, and 47.4% were female. The median age of study population was 36 years. ... nasal bleeding in 1 case, and loosening of teeth in 1 case. Ear-related complaints were present in 10.3% of the total patients. ... and one patient developed a surgical site infection that was managed ...
Objective This study aims to examine the clinical characteristics and surgical management of pediatric testicular epidermoid cysts, thereby contributing to the existing body of knowledge pertinent to the diagnosis and therapeutic intervention 你 s for this condition. Methods A retrospective analysis was conducted on the clinical records of 23 pediatric patients diagnosed with testicular ...